

2026-05-04
Posterior Tooth Inclination, Headaches, and TMD: What’s the Link?
By Agatha Bis, DDS
TMJ Whisperer Academy
The clinical intersection of dental architecture, specifically the buccolingual inclination of the posterior dentition, and the physiological regulation of the masticatory muscles provides a critical framework for understanding chronic cephalgia and temporomandibular disorders (TMD). For decades, practitioners have observed that patients presenting with persistent tension-type headaches or migraines frequently exhibit a distinct morphological configuration: a generalized lingual inclination of the mandibular molars and premolars, often coupled with varying degrees of mandibular retrusion.¹ This structural arrangement, when evaluated through the lens of the Mandibular Entrapment Hypothesis, suggests that the physical orientation of the teeth acts as a mechanical constraint, effectively trapping the mandible and preventing it from following its neuromuscularly preferred trajectory during functional and parafunctional excursions.¹
Morphological Parameters of Posterior Occlusion
The structural alignment of the human dentition is not arbitrary but follows a complex geometric pattern designed to optimize masticatory efficiency while protecting the supporting structures from non-axial loading. Central to this architecture is the Curve of Wilson, a transverse compensatory curve that describes the inward tilt of the mandibular posterior teeth and the corresponding outward tilt of the maxillary posterior teeth.² Under ideal conditions, this curve facilitates the transition of occlusal forces along the long axes of the teeth and ensures that during lateral jaw movements, the posterior teeth on the non-working side do not interfere with the guidance provided by the anterior teeth and canines.²
Quantitative Analysis of Molar Inclination
Modern diagnostic imaging, particularly Cone-Beam Computed Tomography (CBCT), has allowed for the precise quantification of these inclinations across different skeletal patterns and age groups. Studies have established normative values for buccolingual inclination in untreated adults, providing a baseline for identifying pathological deviations. For instance, in skeletal Class I individuals, the maxillary first molars typically exhibit a buccal inclination of approximately +4.85⁰ ±, whereas the mandibular first molars demonstrate a more pronounced lingual inclination of approximately -12.60⁰ ±.³
These values are subject to significant variation based on the underlying skeletal sagittal pattern. Research indicates that patients with skeletal Class II patterns - characterized by a retrognathic mandible - often show higher degrees of lingual inclination in the mandibular molars compared to Class I and Class III patients.² This compensatory inclination is thought to be an adaptive response to the discrepancy in arch width and position, yet it often introduces the very mechanical interferences that lead to neuromuscular dysfunction.²
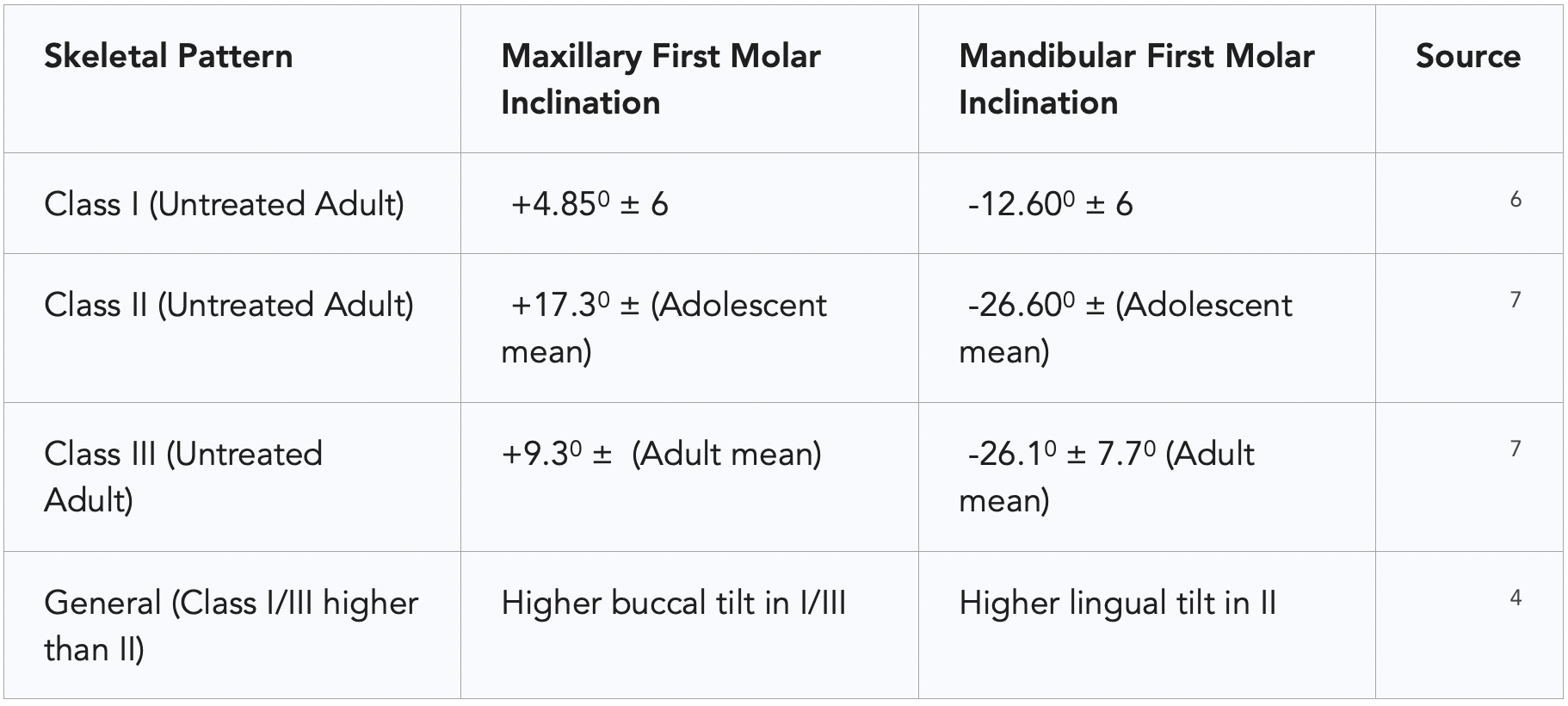
Furthermore, age plays a decisive role in the maturation of these inclinations. Maxillary and mandibular molars tend to "upright" as an individual moves from childhood into adulthood.⁶ In children aged 6 to 9, the mean lingual inclination of mandibular first molars can be as high as -34.9⁰ ±11.0⁰, reducing to approximately -26.1⁰ ±7.7⁰ by age 20 to 35.⁷ When this natural uprighting process is incomplete or when orthodontic intervention fails to establish proper buccolingual torque, the resulting excessive lingual inclination predisposes the patient to balancing interferences and kinematic restriction.¹
Clinical Standards and the ABO Guidelines
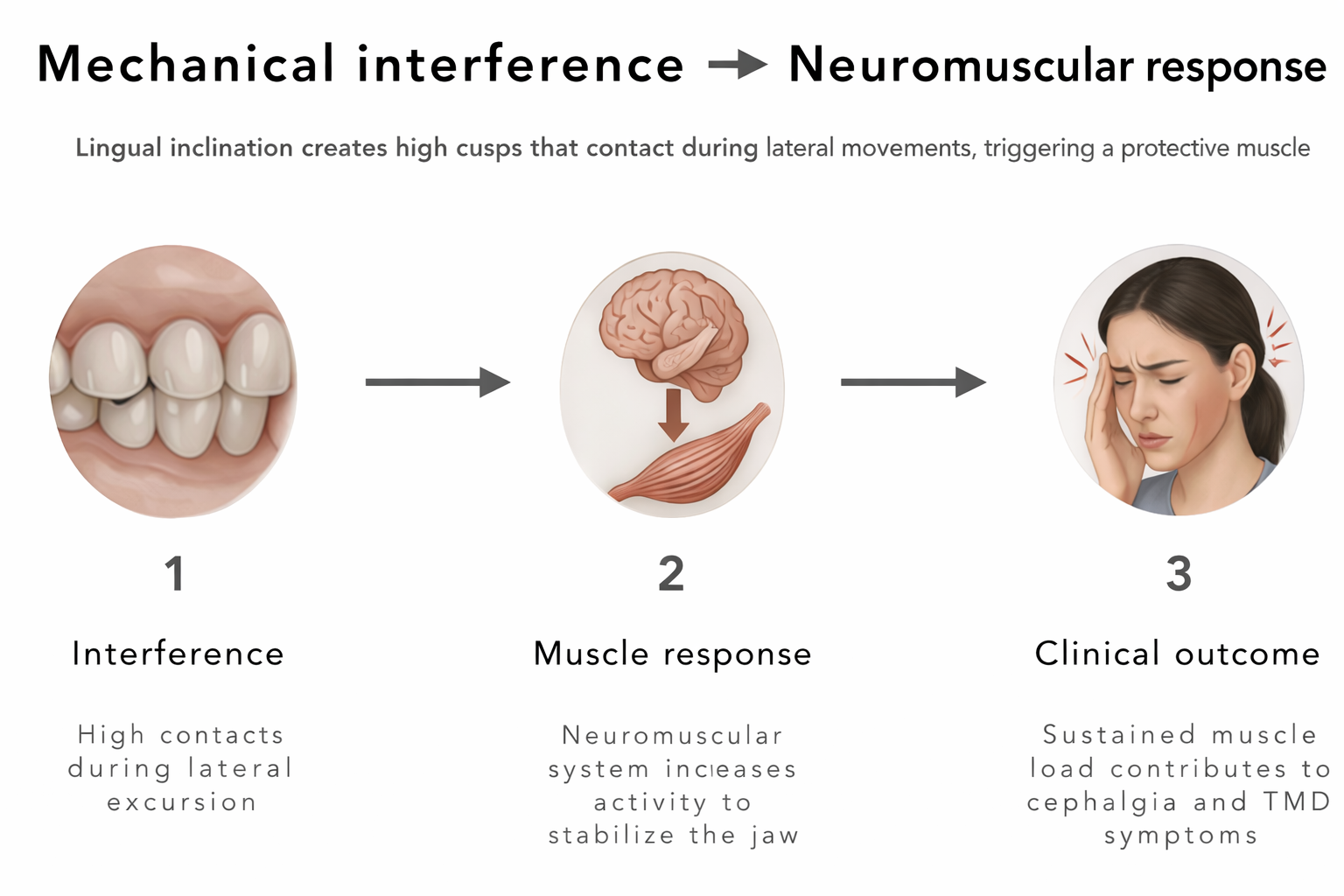
The American Board of Orthodontics (ABO) has established clear criteria for what constitutes a finished and stable occlusion. To avoid balancing interferences - which occur when posterior teeth contact during the side of the jaw that is moving away from the midline - the ABO states that there should not be a significant difference between the heights of the buccal and lingual cusps of the molars and premolars.¹ Specifically, in the maxillary arch, a straight edge placed across the lingual cusps should find the buccal cusps within 1mm of the same surface.⁵ Similarly, in the mandibular arch, the lingual cusps should be within 1mm of the surface defined by the buccal cusps.⁵ Deviations from these standards create "high" cuspal landmarks that prematurely engage during lateral excursions, triggering a defensive neuromuscular response.¹
The Mandibular Entrapment Hypothesis
The Mandibular Entrapment Hypothesis posits that the generalized lingual inclination of the posterior dentition, particularly when paired with a retrognathic mandible, creates a physical cage for the jaw.¹ In a physiologically balanced system, the mandible should be able to move freely into lateral excursions, guided by the canines and incisors, with the posterior teeth separating (discluding) almost immediately. However, when the mandibular teeth tilt inward and the maxillary teeth follow with a corresponding buccal tilt, the posterior cusps remain in contact for an extended duration during these movements.¹
Kinematic Restriction and Muscle Recruitment
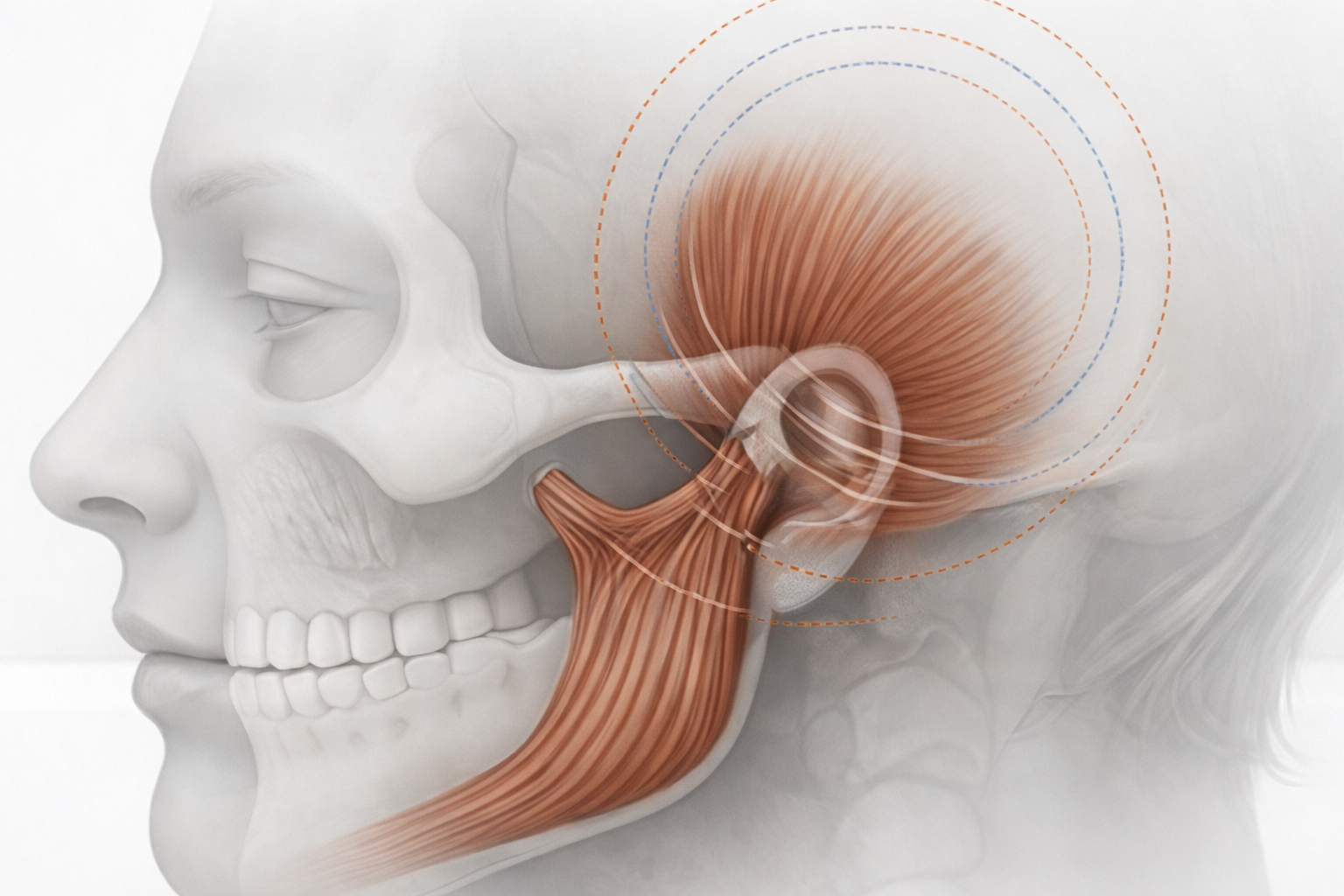
This mechanical constraint is not merely a dental issue but a neurological trigger. The mandible possesses a neuromuscularly preferred position - a trajectory of movement that is most efficient for the muscles and joints. When the dental architecture dictates a "permissible path" that differs from this preferred trajectory, a state of chronic conflict arises.¹ The muscles of mastication, primarily the temporalis and masseter, must work harder to navigate the jaw around these dental interferences. This leads to chronic masticatory muscle hyperactivity, which manifests clinically as tension-type headaches or migraines.¹
In patients with mandibular retrognathism, the situation is exacerbated by altered muscle recruitment patterns. Research by Throckmorton et al. has demonstrated that retrognathic subjects do not recruit their jaw muscles with the same precision as normal subjects; instead, the muscles tend to function as a less-coordinated unit during positioning movements.¹ These individuals often show decreased muscle efficiency, meaning that for any given amount of bite force produced, their muscles exhibit higher levels of electrical activity.¹⁰ When this inefficient system is forced to contend with the mechanical "trap" of lingual inclination, the threshold for pain and dysfunction is rapidly exceeded.¹
Morphological Indicators of Trauma
The existence of mandibular entrapment can often be inferred from specific wear patterns and lesions on the teeth, which act as a "morphological record" of habitual movement trajectories.¹ Key indicators include:
Canine Wear Facets: The presence of significant wear on the canines is often a sign that the anterior guidance system is being overwhelmed by posterior interferences.¹
Abfractions and Non-Carious Cervical Lesions (NCCLs): These wedge-shaped defects at the gumline are caused by the flexure of the tooth under lateral occlusal forces.¹² As the tooth is "trapped" and subjected to oblique loads, the stress concentrates at the cervical region, rupturing the chemical bonds between hydroxyapatite crystals.¹²
Gingival Recession: Often occurring concurrently with abfractions, recession is a biological response to the chronic mechanical stress of lateral forces.¹
Scientific investigations using three-dimensional finite element analysis have confirmed that oblique loading - typical of the forces generated in an "entrapped" mandible - produces significantly higher stress and strain values in the cervical region of teeth compared to axial loading.¹³ For instance, a 100N load applied at a 45⁰ angle to the long axis of a maxillary premolar can produce peak tensile stresses that lead to microfractures in the enamel and dentin.¹³
Neurophysiological Cascades and Muscle Hyperactivity
The link between dental contact and muscle contraction is mediated by the periodontal ligament (PDL) mechanoreceptors.¹⁵ These specialized receptors are embedded in the connective tissue surrounding the roots of the teeth and are sensitive to the slightest pressure. When teeth come into contact, the PDL mechanoreceptors send signals to the central nervous system (CNS), specifically the trigeminal motor nucleus, which in turn regulates the firing of the masticatory muscles.¹⁵
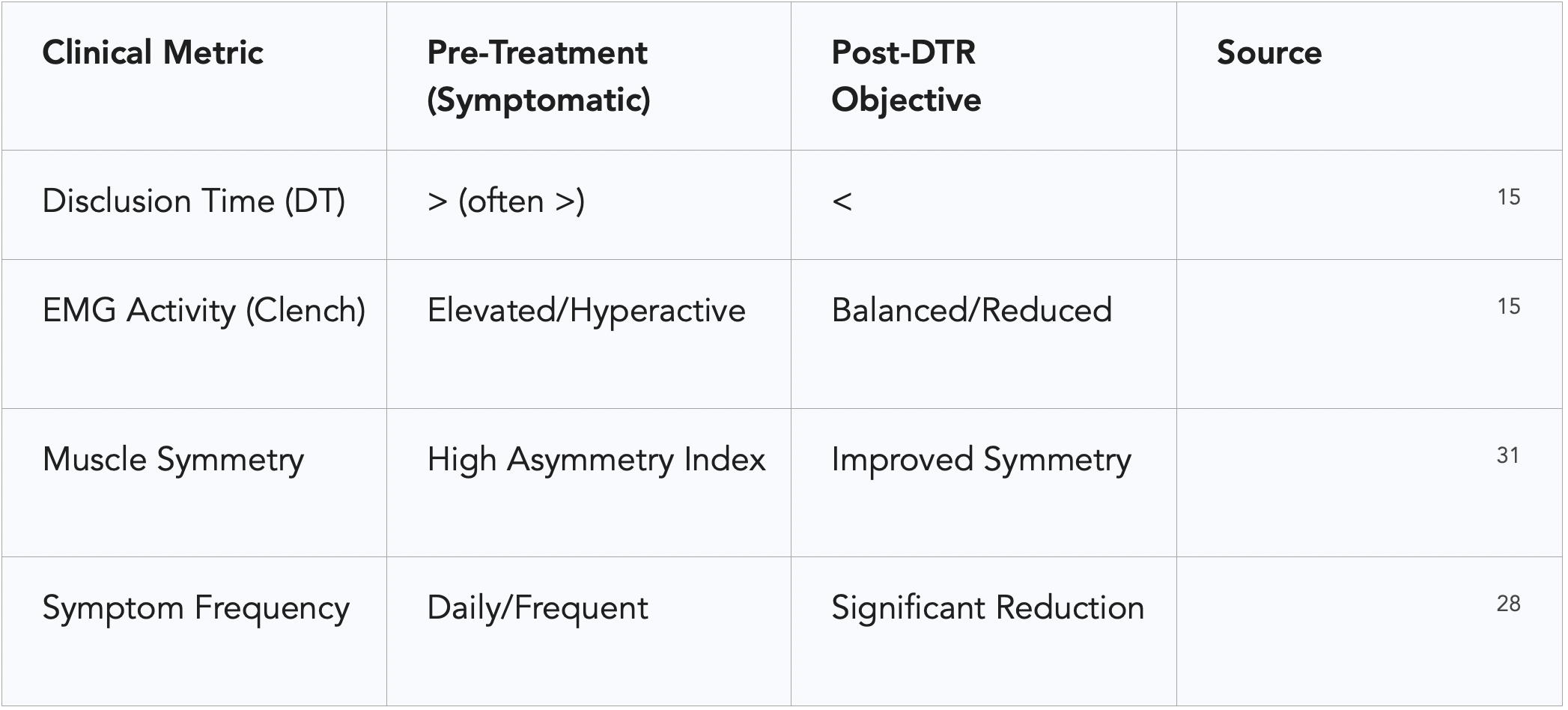
A critical metric in this neurophysiological loop is "Disclusion Time" (DT). DT is defined as the duration required for all posterior teeth (molars and premolars) to separate from each other during a mandibular excursion that begins from a state of complete intercuspation.¹⁵ In a healthy, asymptomatic individual, the disclusion time is typically less than 0.5 seconds, and ideally less than 0.4 seconds.¹
When the disclusion time is prolonged - due to lingual inclination or other occlusal interferences - the PDL mechanoreceptors are subjected to sustained compression. This continuous sensory input signals the CNS to keep the masticatory muscles in a state of high activity.¹⁵ This hyperactivity is not a voluntary action but a reflexive "protective co-contraction" intended to shield the interfering teeth from further trauma.²² However, the unintended consequence of this sustained contraction is muscle ischemia - a reduction in blood flow that leads to a lack of oxygen and an accumulation of lactic acid and other metabolic waste.¹⁵ It is this ischemic state that produces the characteristic dull, aching pain of tension headaches and can trigger the neurological cascade associated with migraines.¹⁵
Muscle Adaptation and Fiber-Type Transition
The masticatory muscles are remarkably versatile and capable of adapting their anatomical characteristics to functional demands.²³ Prolonged hyperactivity and resistance-type training (as seen in chronic clenchers or those with restricted kinematics) can lead to muscle hypertrophy, characterized by an increase in the cross-sectional area of muscle fibers and a higher mitochondrial content.²³
More importantly, muscle fibers can undergo phenotype transitions. Increased muscular activity often elicits a transition toward slower, more fatigue-resistant fiber types (MyHC-IIX ⟶ MyHC-IIA ⟶ MyHC-I).²³ While this might seem beneficial, the chronic engagement of these fibers without adequate rest periods leads to the development of myofascial trigger points and persistent pain.²³ Conversely, when neuromuscular activity is reduced - such as after a successful occlusal correction - these changes are reversible, allowing the muscle to return to a more physiologic state.²³
Disclusion Time Reduction (DTR) and the ICAGD Protocol
The recognition of prolonged disclusion time as a primary etiological factor in muscular TMD and headaches has led to the development of Disclusion Time Reduction (DTR) therapy.¹⁵ DTR is a measurement-driven, computer-guided clinical protocol designed to identify and eliminate the specific tooth contacts that prevent rapid posterior disclusion.¹⁵
Digital Diagnostic Technology
The efficacy of DTR is entirely dependent on objective biometric data. Traditional methods of occlusal analysis, such as the use of articulating paper, are insufficient for this purpose. Articulating paper only provides information about the location of a contact; it cannot quantify the timing or the force.²⁰ Studies have shown that prosthodontists have low clinical accuracy when trying to identify high-force contacts based solely on the size or color of paper marks.²⁷
DTR therapy utilizes two primary technologies:
T-Scan (Digital Occlusal Analysis): This system uses a thin, flexible sensor with a grid of 256 relative force levels.²⁸ When a patient bites on the sensor, the software records a "force movie" that shows the sequence of tooth contacts with a precision of 0.003 seconds.²⁰
M-Scan (Surface Electromyography): A multi-channel surface EMG system that quantitatively records the amplitude and timing of temporalis and masseter muscle activity during both static and dynamic mandibular function. When synchronized with T-Scan data, it enables precise temporal correlation between muscle activation patterns and occlusal contact sequence and force distribution, facilitating objective analysis of neuromuscular response to occlusal loading.²⁴
The Implementation of ICAGD
The clinical procedure used to achieve DTR is known as Immediate Complete Anterior Guidance Development (ICAGD) coronoplasty.¹⁵ ICAGD is a precise enameloplasty protocol where the clinician removes minute amounts of enamel from the posterior teeth to eliminate the interferences that occur during the first fractions of a second of an excursion.¹⁵
The procedure is typically performed in several appointments, allowing the teeth to "rebound" and the muscles to relax between sessions.¹⁹ The ultimate goal is to reduce the disclusion time in both right and left excursions to less than 0.4 seconds.¹⁵ By achieving this rapid disclusion, the clinician effectively "shuts down" the hyperactive signal from the PDL mechanoreceptors, allowing the masticatory muscles to return to a baseline state of rest.¹⁵
Clinical Efficacy and Research Outcomes
The clinical success of DTR therapy in treating headaches and TMD is supported by a growing body of peer-reviewed research, including longitudinal studies and randomized controlled trials (RCTs).
The Randomized Controlled Trial Evidence
A pivotal RCT conducted by Thumati et al. evaluated the effect of DTR on first-year dental students who suffered from muscular TMD and associated emotional depression.²⁹ The subjects were randomly assigned to a treatment group (ICAGD) or a control group (placebo polishing).²⁸
The results were stark. One week after receiving ICAGD, the treatment group showed a dramatic reduction in all outcome parameters, including pain frequency, symptom intensity, and Beck Depression Inventory-II (BDI-II) scores.²⁸ These improvements continued to decline over the six-month observation period.²⁸ In contrast, the control group showed no significant change in their symptoms, and in some cases, their functional restriction scores actually increased.²⁹ This study effectively countered the long-standing belief that TMD is primarily a psychological disorder, demonstrating instead that the emotional distress is often a secondary consequence of chronic physical pain caused by occlusal factors.²⁹
Longitudinal Stability
The longevity of DTR outcomes has also been documented. In a three-year recall study of 100 myofascial pain patients, researchers found that the reduction in symptom intensity achieved on day one of treatment remained statistically significant throughout the entire 36-month period.²¹ This indicates that once the neuromuscular system is "reset" by correcting the disclusion time, the body can maintain this healthier state as long as the occlusal parameters remain stable.¹⁸
Broader Systemic and Neurological Effects
The implications of DTR therapy extend beyond simple muscle pain. Because the trigeminal nerve - the primary sensory nerve for the head and face - is central to the masticatory system, corrections in occlusion can have far-reaching effects.²⁵
Migraine Management: No previously published occlusal adjustment study focused specifically on medically diagnosed migraine patients until the 2021 Thumati study.³² This research found that DTR significantly reduced the frequency and intensity of migraine attacks, likely by reducing the chronic neurogenic inflammation caused by a stressed trigeminal system.¹
Meniere’s Disease and Tinnitus: Retrospective studies have found a high correlation between occlusal DTR treatment and the reduction of symptoms in Meniere’s Disease (MD).²⁴ Patients reported fewer episodes of vertigo and improved tinnitus symptoms, suggesting a link between jaw function and the vestibular apparatus.²⁴
Trigeminal Neuralgia: Even in cases of Trigeminal Neuralgia (TN), which is often thought to be purely a vascular compression issue, DTR has shown promise in reducing the frequency of episodes.²⁴
Postural Stability: There is emerging evidence that occlusion influences whole-body posture and plantar arch pressure.²⁴ Five-year cohort studies have shown changes in postural sway and forward head posture following DTR, indicating that the jaw is a critical link in the body's postural chain.³²
Systemic Health and Inflammatory Implications
Contemporary research is beginning to link poor occlusion and the resulting muscle hyperactivity to broader systemic health issues through the mechanisms of inflammation and oxidative stress.
Neurogenic Inflammation and Cortisol
Chronic stress on the temporomandibular joint and the trigeminal nerve can lead to low-grade neurogenic inflammation.²⁵ This state is often associated with elevated levels of salivary cortisol, a primary stress hormone.²⁵ Studies have shown that TMD patients have significantly higher stress and cortisol levels compared to healthy controls, with the highest levels found in patients with disc displacement and limited mouth opening.³⁴ By balancing the bite forces and reducing EMG activity, DTR therapy helps lower the body's overall inflammatory load and cortisol levels, improving systemic well-being.²⁵
Periodontal Microtrauma and Bacterial Spread
An intriguing second-order insight involves the relationship between occlusion and the integrity of the periodontal barrier. Excessive occlusal forces, such as those seen in bruxism or patients with "entrapped" mandibles, cause microtrauma to the periodontium.²⁵ This can lead to a disruption of the epithelial barrier, potentially allowing oral bacteria such as P. gingivalis and F. nucleatum to enter the bloodstream.²⁵ Thus, DTR therapy may play a role not only in pain relief but also in reducing the risk of systemic inflammation associated with periodontal pathogens.²⁵
Diagnostic Challenges and the Standard of Care Debate
Despite the evidence supporting the link between occlusion and TMD, there is considerable debate within the dental community regarding the standard of care.
The IOS Scanner vs. T-Scan
As digital dentistry advances, intraoral scanners (IOS) are increasingly used to estimate occlusal force through "occlusograms." However, comparative studies have shown that the force estimates from IOS software (like Primescan) do not reliably match the measured relative occlusal force levels from the T-Scan.²⁷ This discrepancy is crucial; if a clinician relies on a scanner's estimate rather than a measured digital reading, they may fail to identify the very interferences that are driving the patient's symptoms.²⁷
Critique of the "10 Key Points"
A recent article by Manfredini et al. proposed "10 Key Points" for treating TMD, which largely downplayed the role of occlusion. However, a coalition of researchers, including Kunte, Sutter, and Thumati, has challenged this, arguing that the Manfredini study lacks scientific support and cannot be considered a standard of care.²⁷ They contend that to presume occlusion is never etiologic of TMD "approaches an absurdity," especially given the high efficacy of DTR and splint therapies in thousands of documented cases.²⁷
Future Outlook and Clinical Recommendations
The evolution of DTR therapy represents a shift toward "Precision Dentistry," where treatment is guided by biometric data rather than subjective clinical judgment. For patients presenting with headaches and lingual inclination, several clinical recommendations emerge from the current literature:
Comprehensive Biometric Screening: Patients with refractory headaches should be screened using T-Scan and BioEMG to evaluate their disclusion time and muscle activity levels.¹⁵
Evaluation of Morphological Indicators: Clinicians should look for abfractions, gingival recession, and canine wear facets as evidence of lateral force trauma.¹
Prioritizing Measurement over Guesswork: The use of articulating paper should be supplemented with digital analysis to ensure that all high-force and late-discluding contacts are identified.²⁷
Integrated Care: Recognizing the link between occlusion and systemic health (e.g., posture, Meniere's, and inflammation) allows for a more holistic approach to patient care.²⁵
In conclusion, the generalized lingual inclination of the posterior dentition is more than an aesthetic or orthodontic concern; it is a mechanical constraint that disrupts the delicate balance of the neuromuscular system. The resulting mandibular entrapment and prolonged disclusion time are primary drivers of chronic muscle hyperactivity, ischemia, and pain. Through the application of Disclusion Time Reduction therapy and the ICAGD protocol, clinicians can measurably restore this balance, providing profound and long-lasting relief for patients suffering from chronic cephalgia and complex temporomandibular disorders. The transition toward objective, computer-guided occlusal adjustment marks a significant advancement in the field, offering hope for patients who have previously been refractory to conventional treatments.
Works cited
Lingually inclined posterior teeth and headaches.pdf
Research Article Buccolingual Inclination of Canine and First and Second Molar Teeth and the Curve of Wilson in Different Sagitt - ScienceOpen, accessed April 3, 2026, https://www.scienceopen.com/document_file/9cfeeb4c-4f32-4999-b05a-4a3a4e620221/PubMedCentral/9cfeeb4c-4f32-4999-b05a-4a3a4e620221.pdf
Buccolingual Inclination of Maxillary and Mandibular First Molars in Untreated Adults: A CBCT Study - IJCMR, accessed April 3, 2026, https://www.ijcmr.com/uploads/7/7/4/6/77464738/ijcmr_2856_v2.pdf
Buccolingual Inclination of Canine and First and Second Molar Teeth and the Curve of Wilson in Different Sagittal Skeletal Patterns of Adults Using Cone-Beam Computed Tomography - ResearchGate, accessed April 3, 2026, https://www.researchgate.net/publication/346686629_Buccolingual_Inclination_of_Canine_and_First_and_Second_Molar_Teeth_and_the_Curve_of_Wilson_in_Different_Sagittal_Skeletal_Patterns_of_Adults_Using_Cone-Beam_Computed_Tomography
Criteria for evaluation of finishing and detailing in orthodontics - MM Publishers, accessed April 3, 2026, https://www.editorialmanager.in/index.php/ijorthrehab/issue/download/10/198
Buccolingual inclination of first molars in untreated adults: A CBCT study - PMC, accessed April 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC8366698/
Buccolingual inclination of molars in untreated children and adults: A cone beam computed tomography study - PMC, accessed April 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC8137116/
Buccolingual Inclination of Second Molars in Untreated Adolescents and Adults with Near Normal Occlusion: A CBCT Study - MDPI, accessed April 3, 2026, https://www.mdpi.com/2077-0383/11/22/6629
Surgical growth modulation for mandibular retrognathism: A case report - J Contemp Orthod, accessed April 3, 2026, https://jco-ios.org/archive/volume/7/issue/3/article/772
Masticatory Function in Retrognathic Patients, before and after Mandibular Advancement Surgery | Request PDF - ResearchGate, accessed April 3, 2026, https://www.researchgate.net/publication/8582073_Masticatory_Function_in_Retrognathic_Patients_before_and_after_Mandibular_Advancement_Surgery
The Use of a BruxChecker in the Evaluation of Different Grinding Patterns During Sleep Bruxism | Request PDF - ResearchGate, accessed April 3, 2026, https://www.researchgate.net/publication/6709974_The_Use_of_a_BruxChecker_in_the_Evaluation_of_Different_Grinding_Patterns_During_Sleep_Bruxism
An Investigation into Non Carious Tooth Wear and Associated Clinical findings Faraedon M., accessed April 3, 2026, https://www.researchgate.net/publication/314097024_An_Investigation_into_Non_Carious_Tooth_Wear_and_Associated_Clinical_findings_Faraedon_M
Effect of root morphology on biomechanical behaviour of premolars associated with abfraction lesions and different loading types | Request PDF - ResearchGate, accessed April 3, 2026, https://www.researchgate.net/publication/261101657_Effect_of_root_morphology_on_biomechanical_behaviour_of_premolars_associated_with_abfraction_lesions_and_different_loading_types
Stresses at the cervical lesion of maxillary premolar - A finite element investigation | Request PDF - ResearchGate, accessed April 3, 2026, https://www.researchgate.net/publication/10929292_Stresses_at_the_cervical_lesion_of_maxillary_premolar_-_A_finite_element_investigation
Disclusion time reduction therapy in treating occluso-muscular pains - PMC, accessed April 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC5308075/
Disclusion Time Reduction (DTR) - ICCMO, accessed April 3, 2026, https://www.iccmo2023india.com/disclusion-time-reduction-dtr/
Effectiveness Of Immediate Complete Anterior Guidance Development In Reducing Disclusion Time In Patients With Chronic Myofascia - IOSR Journal, accessed April 3, 2026, https://www.iosrjournals.org/iosr-jdms/papers/Vol25-issue1/Ser-3/Q2501038695.pdf
The effect of reduced disclusion time in the treatment of myofascial pain dysfunction syndrome using immediate complete anterior, accessed April 3, 2026, https://www.tmdheadacheoregon.com/assets/docs/Thumati20.pdf
DTR Therapy Leading London Experts | Dulwich Dental Office, accessed April 3, 2026, https://dulwichdentaloffice.com/dental-treatments/dtr-therapy/
T-Scan and DTR | Bliss Dental, accessed April 3, 2026, https://www.blissdental.co.uk/t-scan-dtr
The effect of disocclusion time-reduction therapy to treat chronic myofascial pain: A single group interventional study with 3 year follow-up of 100 cases - PMC, accessed April 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC5000572/
Clinical application of a maximum intercuspal position-centric relation occlusion conversion of a lateral cephalogram in the treatment of orthodontic patients | Request PDF - ResearchGate, accessed April 3, 2026, https://www.researchgate.net/publication/352735472_Clinical_application_of_a_maximum_intercuspal_position-centric_relation_occlusion_conversion_of_a_lateral_cephalogram_in_the_treatment_of_orthodontic_patients
The adaptive response of jaw muscles to varying functional demands - Oxford Academic, accessed April 3, 2026, https://academic.oup.com/ejo/article/31/6/596/465295
Prafulla Thumati MDS, Ph D. Head of Department at Rajarajeswari Dental College and Hospital - ResearchGate, accessed April 3, 2026, https://www.researchgate.net/profile/Prafulla-Thumati
Disclusion Time Reduction Treatment - Perfect teeth, accessed April 3, 2026, https://www.perfectteethdental.co.uk/treatments/disclusion-time-reduction-treatment/
DTR Therapy for the Perfect Bite (Occlusion) | by Dr. Nick Yiannios - Medium, accessed April 3, 2026, https://medium.com/@cnotmj/dtr-therapy-for-the-perfect-bite-occlusion-d34bb300376a
All Articles tagged T-Scan - Advanced Dental Technologies & Techniques, accessed April 3, 2026, http://adtt.scholasticahq.com/articles?tag=T-Scan
(PDF) A Multi-Center Disclusion Time Reduction (DTR) Randomized Controlled Occlusal Adjustment Study Using Occlusal Force and Timing Sensors Synchronized with Muscle Physiology Sensors - ResearchGate, accessed April 3, 2026, https://www.researchgate.net/publication/356493810_A_Multi-Center_Disclusion_Time_Reduction_DTR_Randomized_Controlled_Occlusal_Adjustment_Study_Using_Occlusal_Force_and_Timing_Sensors_Synchronized_with_Muscle_Physiology_Sensors
A Disclusion Time Reduction Randomized Controlled Occlusal Adjustment Trial - Thumati et al - ADT&T 2020 rev 10, accessed April 3, 2026, https://www.researchgate.net/publication/341057441_A_Disclusion_Time_Reduction_Randomized_Controlled_Occlusal_Adjustment_Trial_-_Thumati_et_al_-_ADTT_2020_rev_10
142 BioEMG Articles Listed in Google Scholar from 2010 to 2025 - Bioresearch, Inc., accessed April 3, 2026, https://bioresearchinc.com/wp-content/uploads/2025/07/142-BioEMG-Articles-in-Google-Scholar-from-2010-to-2025-1.pdf
Electromyographic activity of the jaw muscles and mandibular kinematics in young adults with theoretically ideal dental occlusion: Reference values - PMC, accessed April 3, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC5432089/
Disclusion Time Reduction (DTR) - Advanced Dental Technologies & Techniques, accessed April 3, 2026, https://adtt.scholasticahq.com/section/1151-disclusion-time-reduction-dtr
Roshan THUMATI | Proprietor | Master of Dental Surgery | Dentistry | Research profile - ResearchGate, accessed April 3, 2026, https://www.researchgate.net/profile/Roshan-Thumati
A prospective-single-arm-study-of-salivary-cortisol-changes-in-muscular-temporomandibular-disorders-patients-following-computer-guided-occlusal-adjustments-galley-proof - ResearchGate, accessed April 3, 2026, https://www.researchgate.net/publication/403358221_A_prospective-single-arm-study-of-salivary-cortisol-changes-in-muscular-temporomandibular-disorders-patients-following-computer-guided-occlusal-adjustments-galley-proof