

2026-04-15
Longitudinal Clinical Implications of Botulinum Toxin Type A in the Management of Masticatory Hyperactivity and Masseteric Hypertrophy
By Agatha Bis, DDS
TMJ Whisperer Academy
Longitudinal Clinical Implications of Botulinum Toxin Type A in the Management of Masticatory Hyperactivity and Masseteric Hypertrophy
The therapeutic application of Botulinum Toxin Type A (BoNT-A) for the management of bruxism and the aesthetic reduction of masseteric volume has transitioned from an off-label novelty to a cornerstone of modern maxillofacial and aesthetic practice. While the immediate symptomatic relief of orofacial pain and the cosmetic appeal of a narrowed lower facial third are well-documented, the long-term clinical nuances suggest a high degree of biological and functional adaptation that warrants exhaustive scrutiny.¹ Originally conceived as a transient intervention for focal muscular hyperactivity, BoNT-A is now recognized as a potent neuromodulatory agent that induces a complex cascade of changes across the masticatory complex, the central nervous system, and the underlying skeletal architecture.² This report provides a comprehensive analysis of the physiological, structural, and neurological implications of repeated BoNT-A administration within the masticatory system, synthesizing longitudinal evidence from current clinical practice and the most recent research through early 2026.
The Neurobiological Mechanism of Peripheral Chemodenervation
The clinical utility of BoNT-A is derived from its ability to induce a state of chemical denervation that is both potent and temporary. At the molecular level, the toxin - a 150 kDa protein produced by Clostridium botulinum - targets the neuromuscular junction with high specificity.³ The molecule consists of a heavy chain (≈ 100kDa) and a light chain ( ≈50 kDa) connected by a disulphide bond. Upon injection into the masseter muscle, the heavy chain facilitates binding to high-affinity receptors on the presynaptic nerve terminal. This is followed by receptor-mediated endocytosis, whereby the toxin enters the nerve terminal within a vesicle.⁴
As the vesicle acidifies, the light chain - a Zn²⁺ -dependent endopeptidase - is translocated into the cytosol.⁴ The primary target of this light chain is the Synaptosomal-Associated Protein of 25 kDa (SNAP-25), a core component of the Soluble N-ethylmaleimide-sensitive factor Attachment protein Receptor (SNARE) complex.⁴ By cleaving SNAP-25, the light chain prevents the successful assembly of the SNARE complex, which is essential for the docking and fusion of acetylcholine-containing vesicles with the presynaptic membrane.² This blockade inhibits the exocytotic release of acetylcholine into the synaptic cleft, effectively preventing the activation of post-synaptic nicotinic receptors and the subsequent muscle contraction.²
While this paralysis is temporary - lasting approximately three to six months as the nerve terminal regenerates functional SNAP-25 proteins and develops temporary axonal sprouts - the chronic repetition of this cycle every 12 to 16 weeks creates a state of persistent muscular under-loading and physiological adaptation.¹ The clinical timeline of this effect is well-characterized, with initial onset typically occurring within 2 to 4 weeks, a peak effect observed at 6 to 8 weeks, and a gradual return of function by the third or fourth month.²

Data derived from.²
The Masticatory System as a Centrally Mediated Circuit
One of the most critical nuances in the management of bruxism is the recognition that the condition is not a primary muscle disorder but a centrally mediated phenomenon.¹ Modern diagnostic frameworks categorize bruxism as a rhythmic masticatory muscle activity (RMMA) driven by brainstem networks and influenced by cortical and subcortical pathways.⁵ BoNT-A, while highly effective at reducing the mechanical output (clench force), acts only peripherally and does not address the underlying neurological drive.¹
Research into the "central drive" of bruxism suggests that the inhibitory control of various nuclei in the brainstem, specifically within the trigeminal motor nucleus and the reticular formation, may be compromised in affected individuals.⁶ Disturbances in the glutamatergic (excitatory) and GABAergic (inhibitory) systems have been identified, with evidence suggesting that lower levels of GABA in the brainstem may be a primary driver of the condition.⁶ Furthermore, genetic polymorphisms in serotonergic neurotransmission - such as the HTR2A rs6313 single nucleotide polymorphism - have been linked to a significant increase in the risk of sleep bruxism, indicating that the behavior is deeply rooted in the patient's neurobiology.⁶
The Paradox of Peripheral Treatment for Central Drivers
When BoNT-A is used to paralyze the masseter, the brain's signals to clench or grind persist. This creates a physiological disconnect: the "command" to contract remains, but the "effector" muscle is unable to respond with the intended force.¹ This mismatch leads to several longitudinal considerations that are rarely addressed in clinical marketing. The nervous system seeks alternative pathways to execute the clench command, which may lead to the recruitment of secondary musculature.¹ Furthermore, prolonged lack of feedback from the primary masseter muscle may lead to a reorganization of the central-peripheral network, potentially altering corticomuscular coherence.¹⁰
In some contexts, the reduction of proprioceptive feedback from the masseter may temporarily alleviate the "urgency" of the central drive, similar to the "sensory tricks" observed in focal dystonia management.³ However, if the underlying driver is related to stress, airway obstruction, or neurological dysfunction, the brain may simply "turn up the volume" on the signal, leading to increased activity in non-paralyzed muscles.¹
Clinical Indications and Aesthetic Drivers
The adoption of BoNT-A in the masseter is driven by two distinct but often overlapping motivations: therapeutic relief from bruxism and aesthetic jaw slimming.¹ Bruxism, which affects approximately 22% of the adult population, manifests as involuntary teeth grinding or clenching.² Over time, this chronic hyperactivity leads to masseter muscle hypertrophy (MMH), characterized by a soft swelling near the angle of the jaw that creates a squared or angular facial profile.¹³
Therapeutic Benefits in Bruxism and TMD
For patients suffering from myofascial temporomandibular disorders (M-TMDs), BoNT-A offers a level of relief that traditional treatments, such as occlusal splints or physical therapy, may fail to achieve in severe cases.² Systematic reviews indicate that BoNT-A significantly reduces bite force and pain intensity for 3 to 4 months.² Patients often report improved sleep quality, fewer morning headaches, and a reduction in dental fractures.¹ The therapeutic effect is dose-dependent, with severe cases requiring higher concentrations to achieve meaningful reduction in hyperactive muscle state.²

Data derived from.²
The Cosmetic Crossover and Social Media Trends
The aesthetic application of BoNT-A for "V-line" contouring or "face slimming" has seen an explosion in popularity, fueled largely by social media platforms.¹ In many East Asian populations, a narrower, more ovoid lower face is considered aesthetically desirable, leading to widespread use of BoNT-A in healthy individuals without significant bruxism.¹⁹ This cosmetic driver has led to the standardization of injection protocols that prioritize volume reduction over functional modulation.² However, clinicians must distinguish between benign masseteric hypertrophy and other causes of facial swelling, such as parotid gland issues or dental infections, to avoid inappropriate treatment.²¹
Long-term Morphological and Structural Muscle Changes
Chronic administration of BoNT-A into the masseter leads to progressive atrophy that may not fully recover between injection cycles.¹ Longitudinal ultrasound studies have quantified this reduction, showing that repeated injections result in a cumulative decrease in muscle thickness.⁸ Even when the neurotoxin's paralytic effect wears off, the muscle volume often remains below the pre-treatment baseline, a phenomenon that can be leveraged for long-term aesthetic maintenance with decreasing doses.¹³
Histological Transformation and Steatosis
The atrophy induced by BoNT-A is not merely a reduction in muscle fiber size; it involves fundamental changes in the histological composition of the muscle tissue.¹⁵ Research has observed the replacement of contractile muscle fibers with fatty and connective tissue, a process known as steatosis.¹⁵ This transformation has significant implications for the long-term functional integrity of the masticatory system. If the contractile capacity of the masseter is permanently diminished through fatty infiltration, the patient may face a lifetime of altered chewing mechanics and reduced bite force, even after treatment is discontinued.¹
Studies involving the flexor digitorum muscles of musicians treated for focal hand dystonia have shown that weakness and atrophy can persist for up to 3.5 years after the cessation of BoNT-A injections.²⁷ This suggests that the "reversibility" of Botox may be a relative term when applied to chronic, high-dose protocols in the masticatory muscles.¹
Compensatory Temporalis Hypertrophy
As the masseter muscle weakens, the temporalis muscle - the other primary elevator of the mandible - frequently undergoes compensatory hypertrophy to maintain masticatory function.⁸ This secondary effect is a common unintended consequence of masseteric chemodenervation.
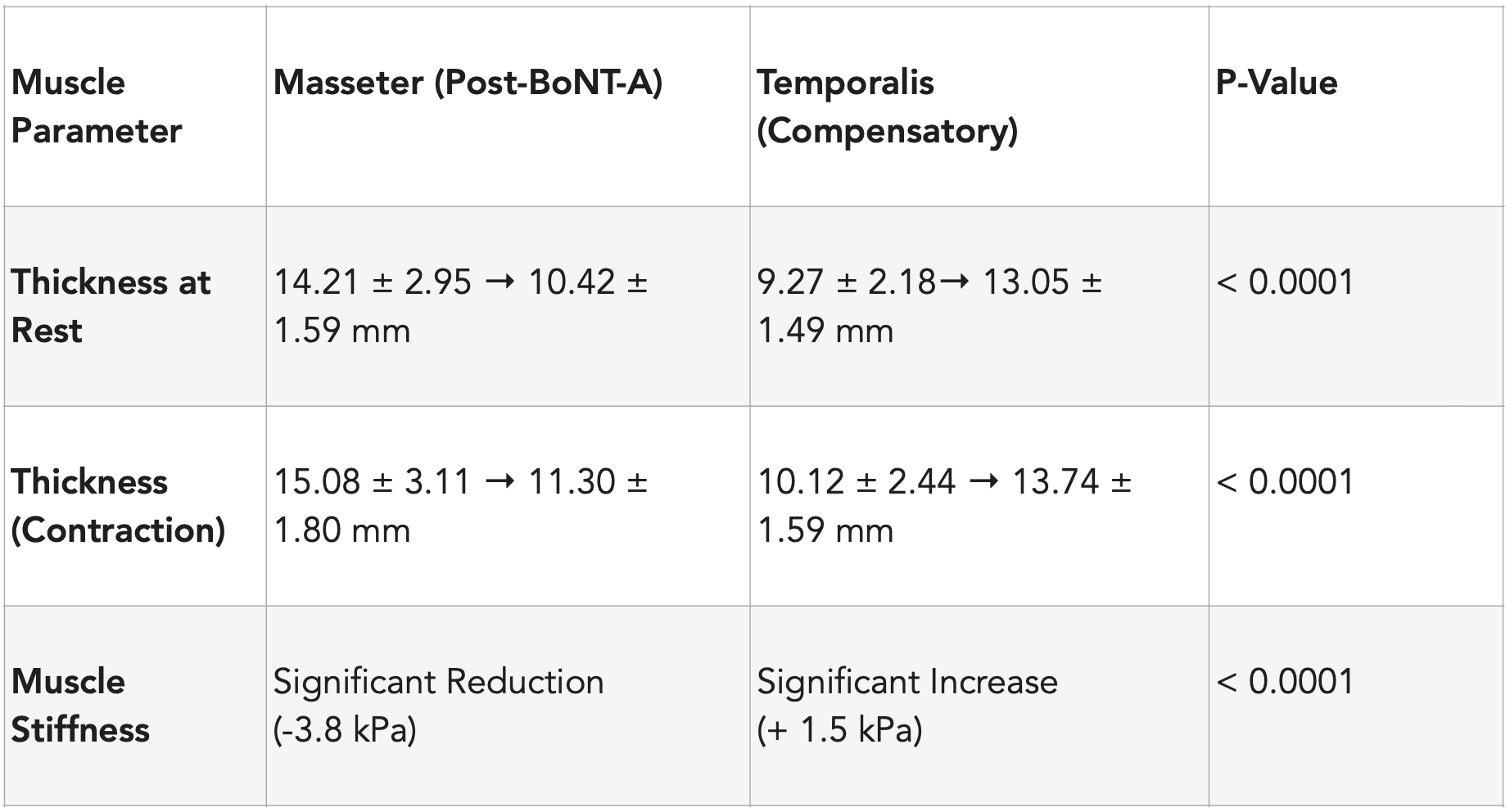
Data synthesized from.⁸
This compensatory thickening typically peaks around 8 to 12 weeks post-injection, coinciding with the nadir of masseteric strength.⁸ For patients seeking aesthetic improvement, this may result in "temporal bulging," where the temples become more prominent as the lower jaw slims.²⁸ In many cases, this necessitates additional injections into the temporalis muscle to maintain facial harmony, creating a broader area of chemodenervation and potentially exacerbating the shift in functional load to the pterygoid muscles or cervical spine.¹
Skeletal Implications and the Mandibular Bone Density Controversy
The impact of long-term masseteric BoNT-A use on the mandibular bone remains one of the most debated topics in maxillofacial research.²⁶ According to Wolff's Law, bone tissue remodels in response to the mechanical loads placed upon it. A chronic reduction in the force exerted by the masseter should lead to a reduction in bone density and volume, a concept supported by extensive animal research.¹
The Disuse Osteopenia Model in Animals
In rodent and rabbit models, the evidence of bone loss following BoNT-A injection is profound. Studies have demonstrated significant reductions in cortical thickness and trabecular density in the mandibular condyle and the alveolar bone.²⁵ These changes occur rapidly, with noticeable decreases in bone volume fraction (BVF) and bone mineral density observed within weeks of a single injection.³³ The persistent under-loading of the jaw joint in these models suggests a risk of disuse osteopenia, which may predispose the mandible to fractures or degenerative changes.¹²
Longitudinal Human Data: The 2025 - 2026 Perspective
In contrast to the findings in animal studies, recent longitudinal data in humans present a more complex picture. A landmark study published in the Aesthetic Surgery Journal (January 2026) utilized high-resolution multi-detector computed tomography (MDCT) to monitor bone density changes in 123 healthy adults over a 12-month period.²²
The study design was rigorous, involving repeat treatments and dose escalation ranging from 48 to 96 units total. The results indicated no clinically significant changes in the bone density of the condyle, premolar area, or ramus compared to baseline or placebo groups.²² This suggests that the human mandible may be more resilient to the reduction in masseteric load than animal models suggest, perhaps due to the ongoing loading from other masticatory muscles like the temporalis and medial pterygoid.²²
However, other researchers argue that a 12-month window is insufficient to observe the cumulative effects of decades of use.³² Some retrospective studies have noted region-specific reductions in the fractal dimension (FD) of the mandibular angle, indicating a more porous or less complex trabecular architecture in long-term users.³⁶
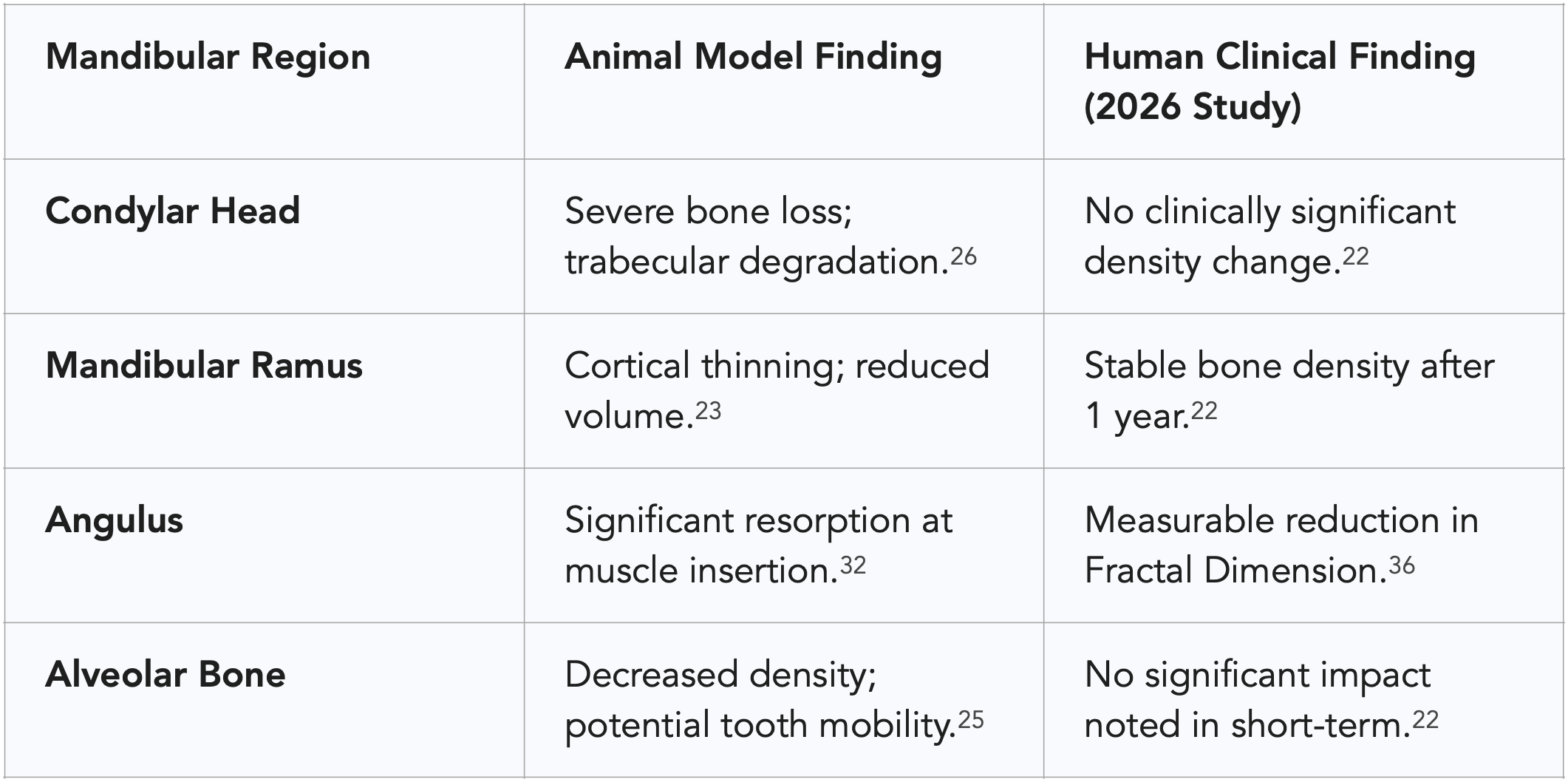
Data synthesized from.²²
Airway Management and Obstructive Sleep Apnea (OSA)
One of the most clinically significant nuances in the management of bruxism is its relationship with airway patency.¹ Recent research has highlighted a staggering correlation between sleep bruxism and Obstructive Sleep Apnea (OSA), with nearly 74% of sleep bruxism cases associated with respiratory events.¹⁸
The Protective Bruxism Theory
The "protective bruxism" theory suggests that clenching and grinding are often functional adaptations to a compromised airway.⁵ During an apneic event, the brain triggers a micro-arousal that activates the jaw muscles to pull the mandible forward, thereby opening the collapsed airway and restoring permeability.⁵ This rhythmic activity is a physiological reflex meant to prevent suffocation.
When a clinician injects BoNT-A into the masseter to stop grinding, they may inadvertently be disabling this protective mechanism.¹ If the masseter is too weak to pull the jaw forward during an apnea event, the duration or severity of the hypoxia may increase. Clinical case reports have documented patients whose Apnea-Hypopnea Index (AHI) increased from 0 to 84 events per hour as the effects of the toxin peaked, directly demonstrating that the "bruxism" was the primary defence maintaining their airway.⁴¹
The Risk of Masking Underlying Pathology
Because BoNT-A effectively reduces pain and tooth wear, the patient and clinician may believe the condition is "cured" while the underlying sleep disorder remains undetected.¹ This delay in diagnosis is dangerous, as untreated OSA is a major risk factor for hypertension, stroke, and cardiac arrhythmia.³⁹ Clinicians are now urged to implement rigorous screening protocols before administering BoNT-A to any patient presenting with bruxism, ensuring that the clenching is not a reactive symptom of a life-threatening airway issue.⁴⁴
Adverse Effects, Complications, and Clinical Nuances
While BoNT-A is generally considered safe, its use in the masseter is associated with a specific set of complications that range from minor aesthetic issues to significant functional impairment.²
Paradoxical Masseteric Bulging
A unique complication of masseteric injections is paradoxical bulging, which occurs in approximately 5% to 10% of patients.² This manifests as a walnut-sized bulge that appears when the patient bites down, usually within 5 to 10 days of the injection.⁴⁵ This phenomenon is caused by uneven toxin distribution, where the superficial layers of the muscle are paralyzed while the deep layers remain active and contract against the atrophying superficial tissue.² This is more common in patients with very large masseters or those who receive single-point injections instead of a multi-point distribution.²
Smile Asymmetry and Soft Tissue Changes
If the toxin diffuses anteriorly to the risorius or zygomaticus muscles, the patient may experience smile asymmetry or difficulty articulating certain sounds.² Additionally, the reduction of masseteric volume can lead to "sagging" of the lower face in older patients or those with poor skin elasticity.²¹ Without the structural support of the masseter muscle, the overlying soft tissue may descend, worsening the appearance of jowls or sunken cheeks.²¹
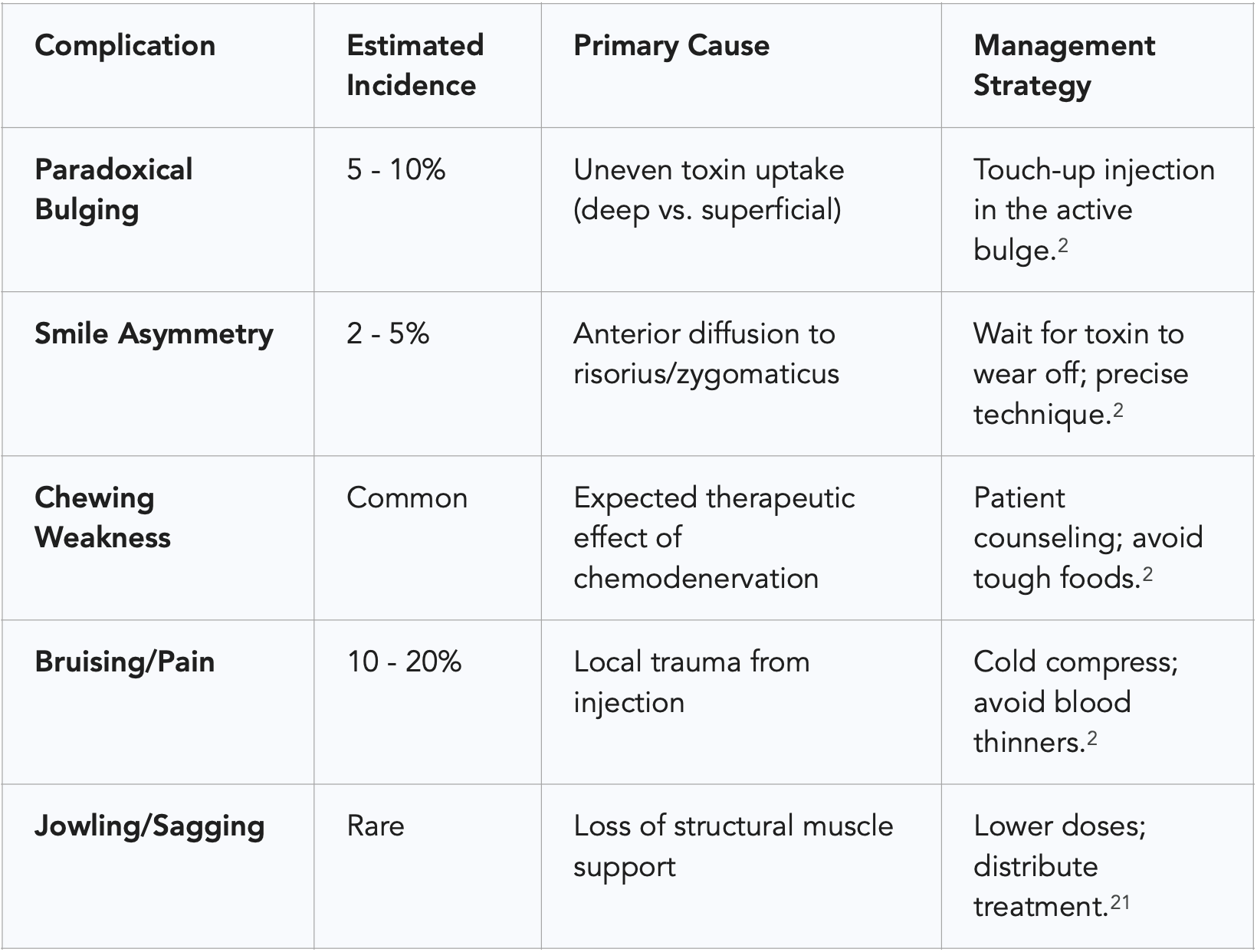
Data derived from.²
Long-term Functional Trade-offs and Joint Stability
The reduction of masseteric force fundamentally changes how the mandible is stabilized during functional and parafunctional activity.¹ For many patients, jaw clenching is a compensatory behavior meant to stabilize a joint that is hypermobile or a bite that is poorly aligned.¹²
The Hypermobility and Joint Instability Risk
Patients with joint hypermobility, such as those with Ehlers-Danlos Syndrome (EDS), often rely on their masseter muscles as "dynamic ligaments" to hold their TMJ in place.¹² For these individuals, weakening the masseter with BoNT-A can lead to increased TMJ clicking, a higher risk of jaw subluxation, and worsening of facial pain as the actual ligaments are forced to take on loads they cannot handle.¹² This highlights the importance of a thorough physical assessment of joint mechanics before initiating paralysis-based therapy.¹²
Occlusal Stability and Proprioception
The resting position of the mandible is maintained by a delicate balance of muscle tone and proprioceptive feedback.⁴⁷ By altering masseteric tone, BoNT-A can shift this balance, potentially leading to subtle changes in tooth position or a "heavy" feeling in the bite.² In some patients, this may lead to "proprioceptive searching," where they grind harder in an attempt to find their occlusal "home," paradoxically worsening the condition.¹
Regulatory Status and the Future of Masseteric Modulation
As of early 2026, the use of BoNT-A for masseteric hypertrophy remains off-label in many Western jurisdictions, but the regulatory landscape is rapidly shifting.¹ In September 2024, China approved BoNT-A specifically for Masseter Muscle Prominence (MMP), following Phase 3 clinical trials that demonstrated high efficacy and safety.²⁰ In the United States, several Phase 3 clinical trials (e.g., NCT06387394, NCT06399718) are in the final stages of data analysis, which may lead to formal FDA approval for the aesthetic indication in the near future.⁵⁰
Synthesis of Long-term Clinical Outcomes
The decision to treat bruxism or masseteric hypertrophy with BoNT-A involves a sophisticated weighing of immediate therapeutic benefit against long-term physiological and structural costs. The longitudinal evidence suggest that while BoNT-A is a powerful tool, it is not a cure and should not be used as a standalone monotherapy in the majority of cases.¹ The "success" of the treatment - measured by a lack of jaw pain and a slimmer face - can be deceptive, masking the progression of sleep disorders or irreversible structural changes in the mandibular bone and joints.¹
Final Conclusions and Recommendations
Based on the synthesis of available data, several high-order conclusions can be drawn for professional practice. First, mandatory screening for Obstructive Sleep Apnea is essential before administering BoNT-A for bruxism to ensure that the clenching is not a protective airway reflex.⁵ Second, BoNT-A should be integrated into a multidisciplinary treatment plan that includes physical therapy to manage cervical and temporal compensation.¹² Third, for long-term users, clinicians must be vigilant regarding the potential for permanent muscle steatosis and mandibular bone remodeling, using objective tools like fractal analysis or high-resolution imaging to monitor skeletal health.³²
Ultimately, the masseteric system is an adaptive, load-bearing complex that maintains its health through function. By selectively paralyzing its primary motor, clinicians are engaging in a long-term modification of the masticatory system that requires ongoing monitoring and a deep understanding of the central-peripheral dialogue. Future management strategies will likely move toward "micro-dosing" and targeted neuro-modulation to balance functional protection with aesthetic desires.¹
Works cited
Bis A. Masseter botulinum toxin injection for bruxism: a clinical perspective on mechanism, limitations, and long-term consequences. TMJ Whisperer Academy. Published April 07, 2026. Accessed April 10, 2026. Available at: https://tmjwhispereracademy.com/resources/masseter-botox-bruxism
Bruxism, Masseter Hypertrophy, and Botulinum Toxin: A Comprehensive Review | Harley Street Institute Journal, accessed March 27, 2026, https://www.harleystreetinstitute.com/journal/bruxism-masseter-hypertrophy-botox-review
Treatment of chronic pain associated with nocturnal bruxism with botulinum toxin. A prospective and randomized clinical study - PMC, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC5268105/
Tension to Tranquility: Treating Awake Bruxism | BOTOX® - Med Supply Solutions, accessed March 27, 2026, https://www.medsupplysolutions.com/blog/botulinum-toxins/treating-awake-bruxism-with-botox/
Botulinum toxins for sleep bruxism - PMC, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11025494/
The neural substrates of bruxism: current knowledge and clinical implications - Frontiers, accessed March 27, 2026, https://www.frontiersin.org/journals/neurology/articles/10.3389/fneur.2024.1451183/full
Hyperexcitability of brain stem pathways in cerebral palsy | Journal of Neurophysiology, accessed March 27, 2026, https://journals.physiology.org/doi/full/10.1152/jn.00185.2018
Temporal Muscles Thicken Compensatorily After Injection of ..., accessed March 27, 2026, https://pubmed.ncbi.nlm.nih.gov/40233307/
Temporalis Muscle Changes Following Botulinum Toxin A Injections ..., accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11541289/
Botulinum toxin combined with rehabilitation decrease corticomuscular coherence in stroke patients | Request PDF - ResearchGate, accessed March 27, 2026, https://www.researchgate.net/publication/358017098_Botulinum_toxin_combined_with_rehabilitation_decrease_corticomuscular_coherence_in_stroke_patients
(PDF) Association of Botulinum toxin treatment due to aesthetic corrections in the face with the level of happiness, anxiety and depression - ResearchGate, accessed March 27, 2026, https://www.researchgate.net/publication/394313958_Association_of_Botulinum_toxin_treatment_due_to_aesthetic_corrections_in_the_face_with_the_level_of_happiness_anxiety_and_depression
Why Botox Shouldn't Be Used Long-Term for TMJ Disorders & Masseter Pain, accessed March 27, 2026, https://cityphysio.com.au/blog/why-botox-shouldnt-be-used-long-term/
The Role of Botulinum Toxin for Masseter Muscle Hypertrophy: A Comprehensive Review, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11860558/
The Role of Botulinum Toxin for Masseter Muscle Hypertrophy: A Comprehensive Review, accessed March 27, 2026, https://www.mdpi.com/2072-6651/17/2/91
Botulinum Toxin-A for the Treatment of Myogenous Temporomandibular Disorders: An Umbrella Review of Systematic Reviews - PMC, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11289222/
Botulinum Toxin for Bruxism: An Overview - PMC, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC12115368/
Efficacy and Safety of Botulinum Toxin in the Management of Temporomandibular Symptoms Associated with Sleep Bruxism: A Systematic Review - PMC, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11203296/
How Sleep Apnea and Teeth Grinding Damage Your Dental Work ..., accessed March 27, 2026, https://bajarsdental.com/how-sleep-apnea-and-teeth-grinding-damage-your-dental-work-what-you-need-to-know-in-2026/
Facial volume reduction and masticatory function after masseter botulinum toxin injection: a prospective study - PMC, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC12512921/
Allergan Aesthetics Launches BOTOX® Cosmetic (onabotulinumtoxinA) for Masseter Muscle Prominence (MMP) in Adults in China - Sep 11, 2024 - AbbVie News Center, accessed March 27, 2026, https://news.abbvie.com/2024-09-11-Allergan-Aesthetics-Launches-BOTOX-R-Cosmetic-onabotulinumtoxinA-for-Masseter-Muscle-Prominence-MMP-in-Adults-in-China
Masseter Hypertrophy Facial Swelling Botulinum Toxin Treatment, accessed March 27, 2026, https://iowaprotocols.medicine.uiowa.edu/protocols/masseter-hypertrophy-facial-swelling-botulinum-toxin-treatment
Longitudinal Computed Tomography Indicates No Negative Impact of OnabotulinumtoxinA on Mandibular Bone Density in a 12-Month - Oxford Academic, accessed March 27, 2026, https://academic.oup.com/asj/articlepdf/46/1/76/64106350/sjaf167.pdf
Repeated injections of botulinum toxin into the masseter muscle induce bony changes in human adults: A longitudinal study - PMC, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC5466904/
Botox Therapy for Hypertrophy of the Masseter Muscle Causes a Compensatory Increase of Stiffness of Other Muscles of Masticatory Apparatus - Semantic Scholar, accessed March 27, 2026, https://www.semanticscholar.org/paper/Botox-Therapy-for-Hypertrophy-of-the-Masseter-a-of-Mierzwa-Olchowy/ce061ee65d4cdb621beb78f2cc3b04a57ef51fce
Mandibular Bone Loss after Masticatory Muscles Intervention with Botulinum Toxin: An Approach from Basic Research to Clinical Findings - PMC, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC6409568/
Botulinum toxin in masticatory muscles: Short- and long-term effects on muscle, bone, and craniofacial function in adult rabbits - PMC, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC3278508/
Long-Term Muscular Atrophy and Weakness Following Cessation of Botulinum Toxin Type A Injections in the Flexor Digitorum Muscle of Musicians with Focal Hand Dystonia - PMC, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC10144778/
Anatomical Considerations When Treating Compensatory Hypertrophy of the Upper Part of the Masseter after Long-Term Botulinum Neurotoxin Type A Injections - PMC, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC7150825/
Botox Therapy for Hypertrophy of the Masseter Muscle Causes a Compensatory Increase of Stiffness of Other Muscles of Masticatory Apparatus - ResearchGate, accessed March 27, 2026, https://www.researchgate.net/publication/361127433_Botox_Therapy_for_Hypertrophy_of_the_Masseter_Muscle_Causes_a_Compensatory_Increase_of_Stiffness_of_Other_Muscles_of_Masticatory_Apparatus
Adverse effect of botulinum toxin-A injections on mandibular bone: A systematic review and meta-analysis - PubMed, accessed March 27, 2026, https://pubmed.ncbi.nlm.nih.gov/37668276/
Longitudinal Computed Tomography Indicates No Negative Impact of OnabotulinumtoxinA on Mandibular Bone Density in a 12-Month, Double-Blind, Randomized, Repeat Treatment, Placebo-Controlled Study in Healthy Adults With Masseter Muscle Prominence | Request PDF - ResearchGate, accessed March 27, 2026, https://www.researchgate.net/publication/394847494_Longitudinal_Computed_Tomography_Indicates_No_Negative_Impact_of_OnabotulinumtoxinA_on_Mandibular_Bone_Density_in_a_12-Month_Double-Blind_Randomized_Repeat_Treatment_Placebo-Controlled_Study_in_Health
Literature Review: Bone Effects of Botulinum Toxin Injection to the Masseter Muscle - Dr Tim Pearce, accessed March 27, 2026, https://drtimpearce.com/2025/12/23/literature-review-bone-effects-of-botulinum-toxin-injection-to-the-masseter-muscle/
Botox and Your Jaw: Unforeseen Long-Term Effects - The JawSpine Centre, accessed March 27, 2026, https://thejawspinedoctor.com/botox-and-your-jaw-unforeseen-long-term-effects/
Does injecting botox into the massters affect jaw bone density? Journal time!, accessed March 27, 2026, https://laurengreenbergmd.com/face/does-injecting-botox-into-the-massters-affect-jaw-bone-density-journal-time/
Effect of multiple injections of botulinum toxin into painful masticatory muscles on bone density in the temporomandibular complex - PMC, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC7693250/
Is Mandibular Cortical Bone and Trabecular Microarchitecture Altered by Masseter Botox Treatment? A Quantitative Perspective - PMC, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC12427982/
Is Mandibular Cortical Bone and Trabecular Microarchitecture Altered by Masseter Botox Treatment? A Quantitative Perspective - MDPI, accessed March 27, 2026, https://www.mdpi.com/2075-4418/15/17/2201
Decreased mandibular cortical bone quality after botulinum toxin ..., accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC7046747/
Study Details | NCT03083405 | Selected Disorders and Sleep Bruxism | ClinicalTrials.gov, accessed March 27, 2026, https://clinicaltrials.gov/study/NCT03083405
Theories on possible temporal relationships between sleep bruxism and obstructive sleep apnea events. An expert opinion, accessed March 27, 2026, https://www.lucaguarda.it/wp-content/uploads/2012/03/183-Theories-on-possible-temporal-relationships-between-sleep-bruxism.pdf
Obstructive sleep apnea due to oromandibular dystonia and treated with botulinum toxin, accessed March 27, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC7954059/
TMJ Treatment from Stretches to Surgeries, accessed March 27, 2026, https://tmjpainhurts.com/tmj-treatment-from-stretches-to-surgeries/
The Connection Between Sleep Apnea and Bruxism: Symptoms, Risks, and Treatment Options, accessed March 27, 2026, https://www.fullersleep.com/connection-between-sleep-apnea-and-bruxism
(PDF) General dental practitioners' knowledge and opinions of snoring and sleep-related breathing disorders - ResearchGate, accessed March 27, 2026, https://www.researchgate.net/publication/356177379_General_dental_practitioners'_knowledge_and_opinions_of_snoring_and_sleep-related_breathing_disorders
BOTOX® and Neuromodulators For Persistent Orofacial Pain & Jaw Disorders - Part 3, accessed March 27, 2026, https://www.nytmj.com/professional-newsletter/botox-and-neuromodulators-for-persistent-orofacial-pain-jaw-disorders-part-3/
Surgical Management of Recurrent Temporomandibular Joint Dislocation - Systematic Literature Review and Development of a Treatme - SciSpace, accessed March 27, 2026, https://scispace.com/pdf/surgical-management-of-recurrent-temporomandibular-joint-n23bs1ys94.pdf
Biomechanics of TMJ and Its Clinical Relevance to Orthodontics: A Review. - International Journal of Health Sciences and Research, accessed March 27, 2026, https://www.ijhsr.org/IJHSR_Vol.6_Issue.7_July2016/49.pdf
Occlusal Appliance Therapy for Temporomandibular Joint Disorders: Mechanisms, Efficacy, and Limitations - International Journal of Health & Medical Research, accessed March 27, 2026, https://ijhmr.com/wp-content/uploads/2025/01/3.pdf
Occlusal Appliance Therapy for Temporomandibular Joint Disorders: Mechanisms, Efficacy, and Limitations - ResearchGate, accessed March 27, 2026, https://www.researchgate.net/publication/388049570_Occlusal_Appliance_Therapy_for_Temporomandibular_Joint_Disorders_Mechanisms_Efficacy_and_Limitations
NCT06387394 | A Study to Assess BOTOX Injections in Adult Participants for the Change of Masseter Muscle Prominence | ClinicalTrials.gov, accessed March 27, 2026, https://clinicaltrials.gov/study/NCT06387394
A Study to Assess BOTOX Injections for the Change of Masseter Muscle Prominence in Adult Participants - TrialX, accessed March 27, 2026, https://www.trialx.com/clinical-trials/listings/290571/a-study-to-assess-10/
A Study to Assess BOTOX Injections for the Change of Masseter Muscle Prominence in Adult Participants - AbbVie Clinical Trials, accessed March 27, 2026, https://www.abbvieclinicaltrials.com/study/M21-417
A Study to Assess BOTOX Injections in Adult Participants for the Change of Masseter Muscle Prominence - AbbVie Clinical Trials, accessed March 27, 2026, https://www.abbvieclinicaltrials.com/study/M21-416
Functional Effects of BoNT-A Application in Masseter Muscle in Patients with Symptoms of Bruxism - MDPI, accessed March 27, 2026, https://www.mdpi.com/2072-6651/17/11/540
The Impact of Botox on the Upper Trapezius: Understanding the Risks and Functions, accessed March 27, 2026, https://www.artevaacupuncture.com/learn/impact-of-botox-on-the-upper-trap