

Introduction: The Cybernetic Loop of Form and Function
The stomatognathic system functions not merely as a mechanical apparatus for mastication but as a complex, biological cybernetic loop where hard tissues (teeth and osseous structures) and soft tissues (muscles, nerves, and ligaments) exist in a state of dynamic, reciprocal interdependence. In the conventional paradigms of clinical dentistry, particularly within the gnathological tradition, the static relationship of teeth has historically dominated diagnostic protocols. Occlusion has been frequently reduced to a study of intercuspation, a geometric puzzle solved on an articulator. However, emerging research and the foundational principles of neuromuscular dentistry suggest that these static relationships are merely the architectural residue of dynamic, functional processes. Central to this evolving understanding is the phenomenon of neuromuscular adaptation, a physiological imperative that becomes particularly acute in patients presenting with mandibular retrusion.
Patients exhibiting a retruded mandible face a fundamental biomechanical and physiological disadvantage. The mandible is positioned posteriorly relative to the cranial base and maxilla, a spatial arrangement that frequently compromises the oropharyngeal airway, compresses the highly innervated and vascularized retrodiscal tissues of the temporomandibular joint (TMJ), and fundamentally alters the optimal length-tension relationships of the masticatory musculature.¹ In response to these noxious inputs, the neuromuscular system does not remain passive. It engages in continuous, albeit metabolically expensive, adaptive remodeling to achieve a mandibular position that minimizes immediate threat, primarily airway obstruction, and maintains essential functions such as respiration, deglutition, and mastication.³
This report considers that dental hard tissue modifications, specifically tooth wear patterns, serve as critical forensic evidence of this adaptive struggle. Far from being random events of attrition or simple mechanical wear, these facets act as "functional records" of the mandible's habitual, compensatory trajectories.³ They reveal the directional vectors where the neuro-musculature attempts to position the mandible, often in direct conflict with the intercuspal position (MIP) dictated by the interdigitation of the teeth. By rigorously analyzing these patterns, specifically the alignment of complementary anterior wear facets, clinicians can approximate a "neuromuscularly preferred" position that differs significantly from, and often corrects, the patient's habitual, pathologic bite.
The Stomatognathic Cybernetic Feedback Loop
2026-03-02
Neuromuscular Adaptation in Mandibular Retrusion: A Comprehensive Analysis of Wear Pattern Diagnostics and Physiologic Mandibular Positioning
By Dr. Agatha Bis
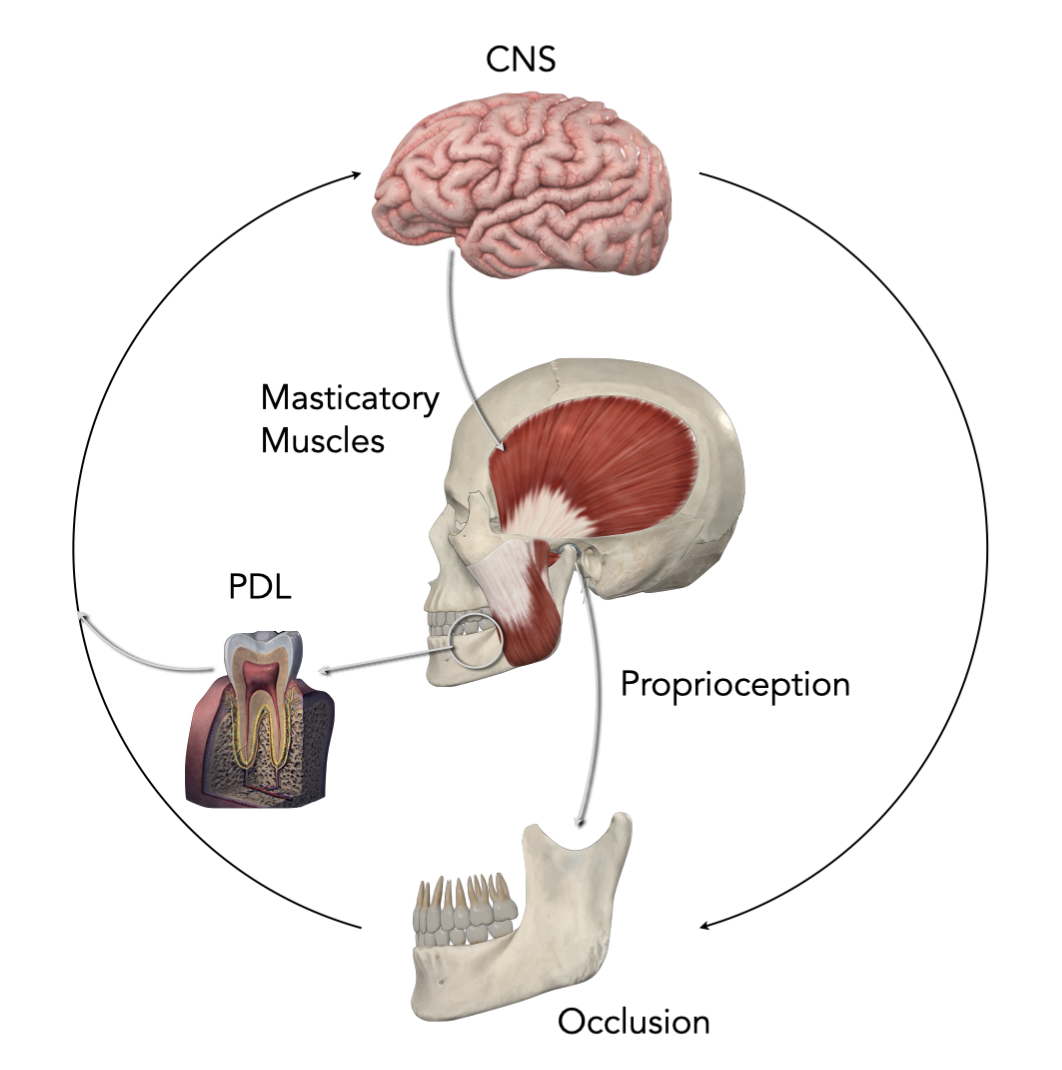
The chewing system works like a feedback loop. Sensory signals from the periodontal ligament (PDL) and the jaw joint (TMJ) send information to the brain. The brain then adjusts how the chewing muscles work. When the lower jaw sits too far back, this feedback system can cause the muscles to adapt and change to make up for structural differences.
The following analysis explores the physiological mechanisms of this adaptation, the diagnostic utility of wear pattern analysis, and the quantification of the spatial discrepancy between habitual and optimal mandibular positions. It integrates foundational theories from neuromuscular dentistry, pioneered by Bernard Jankelson, with contemporary research on electromyography (EMG), kinesiography, and biomechanics to provide a unified theory of mandibular function in the structurally compromised system. It challenges the clinician to look beyond the static intercuspation and see the dynamic neuromuscular reality etched into the enamel.
2. The Biomechanics and Physiology of Mandibular Retrusion
To fully grasp the diagnostic significance of wear patterns, one must first dissect the physiological burden imposed by mandibular retrusion. Mandibular retrusion is characterized not just by the aesthetic profile of a "weak chin," but by the posterior positioning of the mandibular condyle within the glenoid fossa and a distal relationship of the mandibular dentition to the maxilla.¹ This skeletal discrepancy initiates a cascade of compensatory mechanisms that reverberate through the entire stomatognathic system.
2.1. Structural Constraints and the Primacy of Airway Patency
The mandible is not merely a hinge for mastication; it serves as the anterior structural support for the tongue and the pharyngeal airway. In patients with retruded mandibles, the anatomical anchor points for the genioglossus and other suprahyoid muscles are displaced posteriorly. Consequently, the tongue base is forced backward, potentially encroaching upon the oropharyngeal space and increasing the risk of airway resistance or obstruction, particularly during sleep.⁵
Physiologically, the maintenance of a patent airway is critical for survival and supersedes all other stomatognathic functions, including occlusion. The central nervous system (CNS) prioritizes respiration. To prevent airway collapse, the neuromuscular system recruits the suprahyoid and masticatory muscles to posture the mandible anteriorly.⁵ This "protective posturing" creates a fundamental conflict: the skeletal and dental reality (MIP) dictates a posterior position, while the functional and respiratory necessity demands an anterior position. The patient survives in a state of constant tension, oscillating between the structurally dictated bite, defined by the intercuspation of teeth, and the functionally required posture needed to breathe.
2.2. Neuromuscular Compensation Mechanisms: The Cost of Adaptation
The muscles of mastication, primarily the masseter, temporalis, and medial and lateral pterygoids, bear the brunt of this positional discrepancy. In a physiologically ideal system, muscles return to a rest position where the sarcomeres are at an optimal length. At this length, the overlap between actin and myosin filaments is maximized for potential cross-bridge formation, allowing the muscle to generate force efficiently upon demand while expending minimal energy at rest.³ This state is defined as the physiologic rest position.
In mandibular retrusion, this rest position is elusive. The muscles are often forced into a foreshortened or overextended state to maintain the habitual occlusion or to posture the jaw forward for airway maintenance.
Isotonic vs. Isometric Adaptation: The neuromuscular system naturally seeks an isotonic state - a balanced tone where muscles are relaxed and ready for function. However, in retrusion, the system is forced into isometric contraction. The muscles must hold tension without shortening to stabilize the mandible in a non-physiologic position, fighting against gravity and the elastic recoil of tissues.⁸
Hyperactivity and Metabolic Debt: To maintain the retruded intercuspal position (MIP) against the body's drive for a more anterior, airway-protective posture, the retractor muscles (such as the posterior fibers of the temporalis and the digastrics) must remain hyperactive. This continuous hyperactivity leads to significant metabolic consequences: the accumulation of metabolic waste products like lactic acid, the depletion of adenosine triphosphate (ATP), and local hypoxia.³ Over time, this biochemical environment lowers the threshold for nociceptor activation, leading to the chronic pain often diagnosed as myofascial pain dysfunction (MPD) or TMD.
Research utilizing kinesiography indicates that the "neuromuscular trajectory”, the path the jaw takes when propelled by relaxed, unencumbered muscles, often differs significantly from the "habitual trajectory" dictated by the teeth.⁷ In retrusion, the habitual closure creates a distalizing force on the mandible. As the teeth engage, they drive the mandible backward, forcing the condyles posteriorly and superiorly into the retrodiscal tissues. This compression of the bilaminar zone, which is rich in nerves and blood vessels, is a primary mechanism implicated in intracapsular pathology and pain.²
2.3. The Concept of the "Launch Pad" and Trajectory
Bernard Jankelson introduced the critical concept of the "launch pad" to describe the physiologic rest position.⁹ In a healthy stomatognathic system, the mandible rests in a spatial sling of relaxed musculature, suspended by the balanced tonus of the elevators and depressors. All functional movements (swallowing, speech, mastication) initiate from this "launch pad." The mandible accelerates through the interocclusal space (freeway space) along an isotonic trajectory to a terminal contact (myocentric occlusion) and then returns to the launch pad.
In mandibular retrusion, the "launch pad" is fundamentally unstable. The muscles are "at war" with the occlusion.³ Every time the patient swallows (which occurs approximately 2,000 times a day) or clenches, the proprioceptive guidance of the teeth forces the mandible back into the retruded position, resetting the cycle of muscle strain. This repetitive conflict between the muscle's preferred trajectory (anterior/ myocentric) and the tooth-guided trajectory (posterior/habitual) is the engine that drives pathological tooth wear.³ The teeth become the casualties of this neuromuscular battle, worn down as the muscles attempt to erase the interferences that prevent the mandible from reaching its physiologic target.
3. Wear Pattern Analysis: Diagnostic Forensics of the Stomatognathic System
In the absence of advanced electronic instrumentation, the history of this neuromuscular conflict is written on the teeth themselves. Tooth wear is typically categorized into attrition, erosion, and abrasion. However, in the specific context of neuromuscular adaptation and mandibular retrusion, attrition (tooth-to-tooth contact) serves a unique and powerful diagnostic role. The provided research material argues that wear facets are not random speculative events; they are morphological evidence of habitual mandibular trajectories.³ They are the geological record of the mandible's movement over time.
3.1. Wear Facets as Vector Indicators
A wear facet is a specific plane of flattened enamel caused by repetitive movement against an opposing tooth. Unlike the generalized, rounded wear of erosion or the random scratches of abrasion, attrition facets are highly polished, sharply defined, and geometrically distinct.³ They represent the specific pathways (the vectors) that the mandible travels during parafunctional activity, particularly nocturnal bruxism.
The Directional Vector: The orientation of a wear facet reveals the direction of force application. For a patient with a retruded mandible, who exhibits severe wear on the facial aspect of the lower incisors and the palatal (and/or incisal) aspect of the upper incisors, the geometry indicates a repetitive anterior-posterior grinding pattern.³ The mandible is driving forward, engaging the anterior teeth in a protrusive movement.
Functional Choice: The critical diagnostic insight is that these facets often indicate a mandibular position that is substantially more anterior than the patient's maximum intercuspal position (MIP).³ This observation is paramount. It suggests that during unconscious grinding, when cortical control is reduced and the system operates on deeper, reflexive levels, the neuromuscular system attempts to drive the mandible forward. This parafunctional movement is likely a subconscious attempt to seek the more physiologically stable or airway-patent position discussed in Section 2, effectively "grinding in" the occlusion to match the muscle's requirement.
3.2. Confirmation of Parafunctional Bruxism and the Muscle Engram
Wear patterns serve a dual diagnostic function: they confirm the presence of bruxism and, more importantly, reveal its mechanics.³ In this framework, bruxism is often interpreted not merely as a localized dental pathology or solely a central nervous system (CNS) stress release, but as a subconscious, functional adaptation. The CNS creates a muscle engram, a memorized pattern of muscle activity, to navigate the mandibular interferences.¹⁴
When the occlusion is restrictive, as is common in deep bite retrusion cases where the mandible is "trapped" behind the maxilla, the engram becomes destructive. The bruxism represents the muscles attempting to erase the restrictive tooth structure to create freedom of movement. The “Avoidance Pattern” described in neuromuscular literature proposes that the masticatory system alters its movement pathway to bypass painful interferences, but when sleep reduces the sensory feedback threshold, the muscles revert to their preferred trajectory, clashing violently with the restrictive dentition.¹⁵ The resulting wear facets map this collision.
3.3. The Anterior Wear Facet Registration Technique
The most clinically significant application of this theory is the Wear Facet Registration Technique, also referred to as the "wear facet alignment" technique.³ This diagnostic procedure moves beyond static observation to dynamic reconstruction of the patient's functional pathology. It involves identifying and physically matching the complementary wear facets on the maxillary and mandibular anterior teeth.
Detailed Clinical Protocol:
Identification: The clinician performs a meticulous intraoral examination to locate polished, matching facets on the incisal edges of the upper and lower anterior teeth (e.g., the incisal edge of a lower incisor, matching the palatal/ incisal wear on an upper incisor).
De-programming (Optional but Beneficial): While not strictly required for the rough estimate, using a TENS unit or a de-programmer prior to this step can facilitate the maneuver by relaxing the muscles involved.
Alignment: The patient's mandible is guided forward (protruded) from the habitual MIP. The clinician instructs the patient to "find the spot where your front teeth fit together." The mandible is manipulated until these opposing wear facets fit together intimately, lining up the pattern of wear and its related pathology.
Approximation: This aligned position represents the "neuromuscularly preferred" or "target" position. It is the physical manifestation of where the muscles have been driving the mandible during thousands of parafunctional episodes.³
This technique provides a tangible, physical record of where the mandible functions during parafunction, which often stands in stark contradiction to where it sits during passive MIP. It serves as a "clinically accessible approximation" of the optimal physiologic position, providing immediate visual confirmation of the discrepancy without the initial need for complex electronic instrumentation.³ It allows the clinician and the patient to see the "phantom bite" that the muscles are striving to achieve.
Anterior wear facet alignment and mandibular repositioning
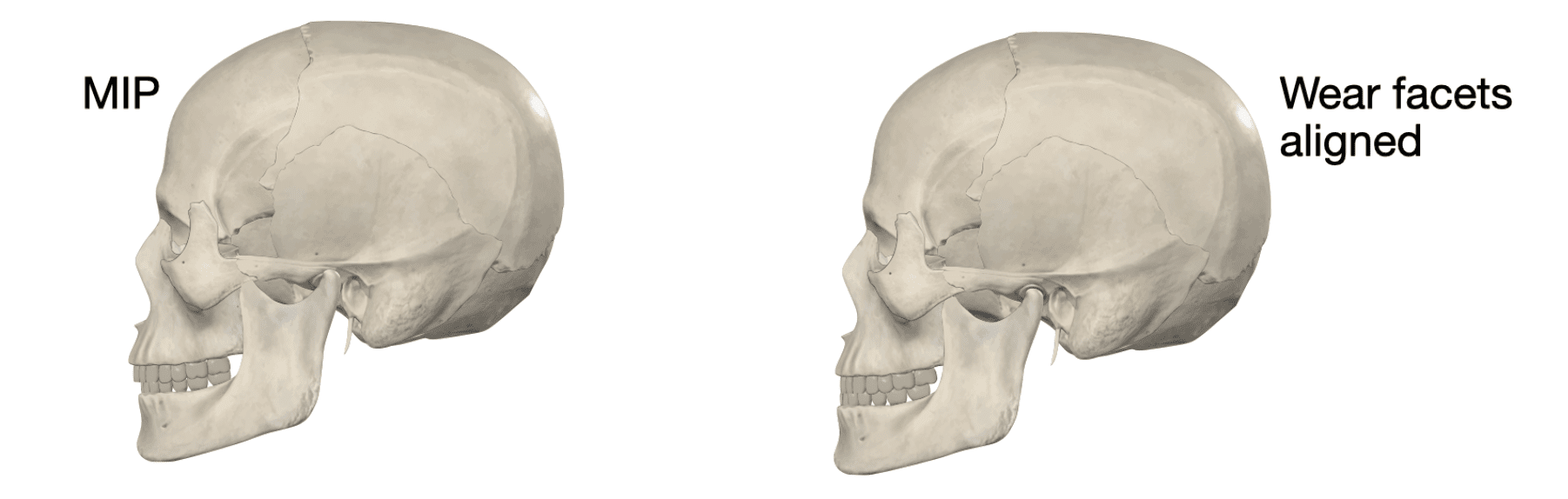
Panel A: The patient is in Maximum Intercuspal Position (MIP). The mandible is positioned posteriorly, causing condylar compression. There is a visible gap between the anterior wear facets.
Panel B: The mandible moves forward to align the matching anterior wear facets. In this “neuromuscular target position,” the condyle shifts anteriorly and the airway opens, highlighting the underlying spatial discrepancy.
4. Quantifying the Spatial Discrepancy: The Mismatch Hypothesis
The core diagnostic value of wear pattern analysis lies not just in identifying the direction of movement, but in quantifying the spatial discrepancy between the habitual bite (MIP) and the neuromuscular target position.³ This discrepancy is the metric of pathology; it represents the "neuromuscular burden" placed on the system.
4.1. Defining the Discrepancy
The analysis identifies two distinct coordinates in the 3D spatial envelope of mandibular motion:
MIP (Maximal Intercuspal Position): The position of maximum tooth contact. In retruded patients, this is a forced posterior position, dictated by the interdigitation of cusps and fossae. It is the "skeletal/dental" reality.
Neuromuscular Target (Myocentric): The position of minimal muscle strain, often approximated by the wear facet alignment. This is the "muscular/ physiologic" reality.
The distance between these two points - the "slide" or "shift" required to move the mandible from the muscle's preferred spot to the tooth's dictated spot - is the spatial discrepancy. The document explicitly states that "the magnitude of this positional discrepancy correlates directly with the severity of musculoskeletal tissue damage and the intensity of associated symptoms".³ A larger slide implies a greater distance the muscles must actively pull the mandible to engage the teeth, and consequently, a higher energy cost.
4.2. Biomechanical Consequences of the Discrepancy
When a significant discrepancy exists (clinical experience and literature often suggest a threshold of 2mm or greater ¹⁶ ), the neuromuscular system is placed in a state of chronic conflict. This conflict manifests in several deleterious biomechanical consequences:
Persistent Hyperactivity: To maintain the teeth in MIP, the muscles cannot relax. They must maintain tonic contraction levels significantly above physiologic resting baseline. This is termed "sustained muscle hyperactivity".³ The muscles act as a splint, holding the jaw in a position that the teeth dictate but the joints and airways reject.
Pathological Joint Loading: As the muscles pull the mandible back from the anterior neuromuscular position to the posterior MIP, the condyles are loaded distally. This loads the condyle against the posterior aspect of the articular disc and the retrodiscal tissues. This chronic, repetitive loading is a primary vector for disc displacement (internal derangement), inflammation (retrodiscitis), and degenerative joint disease (osteoarthritis).¹¹ The wear facets on the anterior teeth are often the mirror image of the compression in the posterior joints.
Threshold of Tolerance: The stomatognathic system possesses a "physiologic tolerance threshold".³ For years, a patient may adapt to this discrepancy via tooth wear, muscle hypertrophy, or postural compensation without overt symptoms. However, adaptation has a metabolic limit. Once the discrepancy exceeds this threshold, often triggered by an acute event like whiplash, stress, or restorative changes that increase vertical dimension or lock the bite further, the system decompensates. Pathology manifests as pain (TMD), restricted range of motion, or fractured dentition.
4.3. Research Validation of Discrepancy and Muscle Activity
Quantitative analysis via electromyography (EMG) provides the biological validation for the wear pattern hypothesis. Data comparing tonic muscle recruitment in the habitual Maximal Intercuspal Position (MIP) versus the Physiologic Rest position (PRP) reveals a stark metabolic contrast. In studies analyzing the masseter and temporalis muscles, the habitual bite in retruded patients consistently demands significantly higher voltage potentials to maintain, indicative of isometric hypertonicity.
Research by Michelotti et al. (1997) is pivotal in this regard. Their study utilized electromyography to investigate mandibular rest positions and found that the average difference between the electromyographic rest position (the true physiologic rest where muscle activity is minimal) and the clinical rest position (often determined by habitual closure) was approximately 6.3 mm.¹⁶ This finding is profound. It suggests that traditional clinical methods often vastly underestimate the "freeway space" required for muscles to achieve true relaxation. A discrepancy of this magnitude (6.3 mm vertically) implies that in the habitual clinical rest, the muscles are still active, holding the jaw closed against its physiologic desire to open further.
Furthermore, Kerstein and Radke (2010) demonstrated the impact of occlusal contact patterns on muscle activity. Their research showed that when anterior guidance (similar to the position found in wear facet alignment) is established and posterior interferences are removed (reducing disclusion time), muscle activity levels in the masseter and temporalis are significantly reduced.¹⁴ Specifically, they found that maximum voluntary clench activity is high in MIP, but the introduction of appropriate anterior contact (without posterior interference) reduces the recruitment of the elevator muscles, essentially "shutting down" the hyperactivity. This supports the concept that the anterior position indicated by wear facets is indeed a position of lower neuromuscular demand.
The data presented in Table 1 below synthesizes the findings regarding the impact of mandibular position on muscle activity, highlighting the "Hyperactivity Gap" created by the discrepancy.
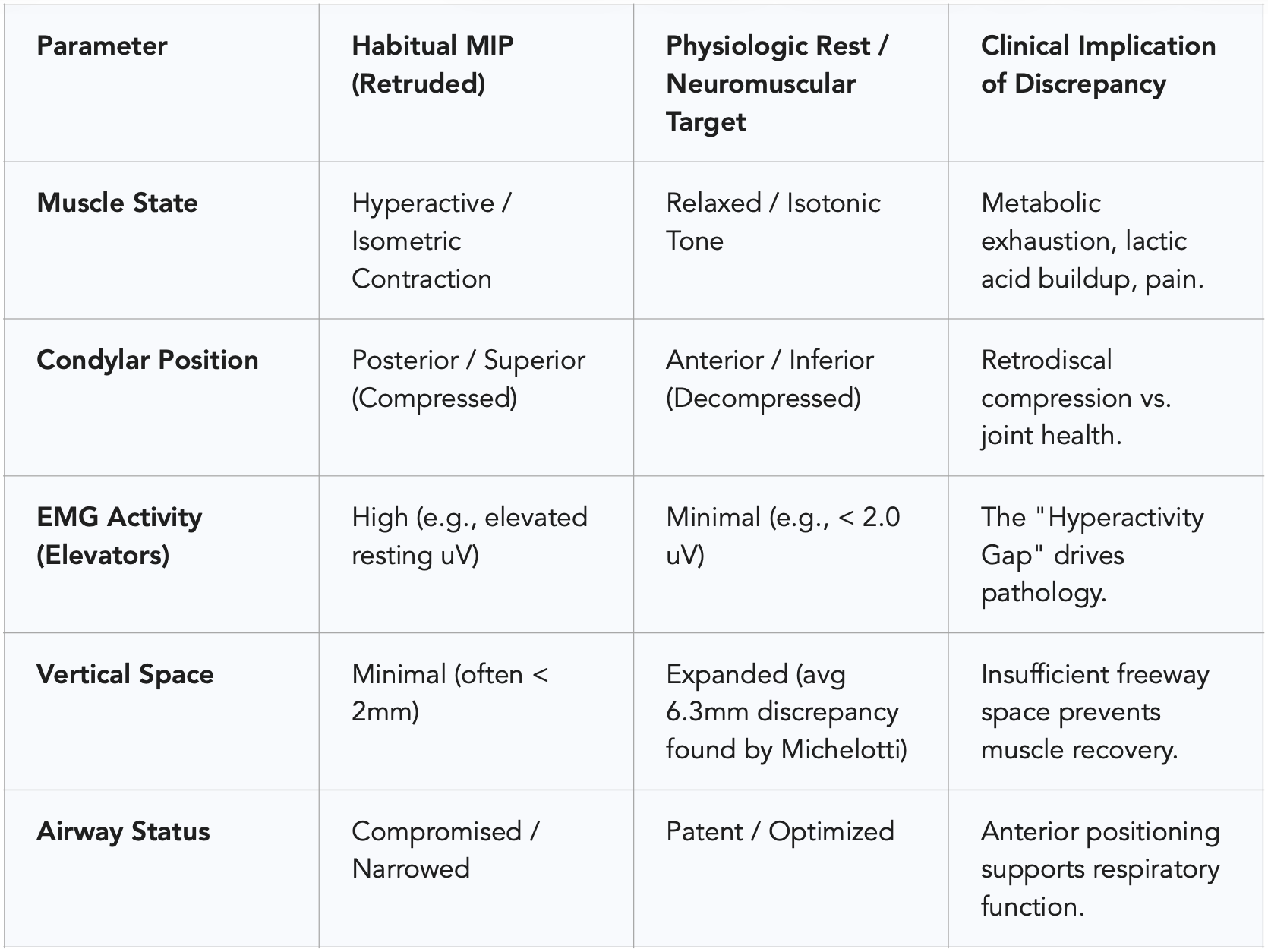
Table 1: Comparison of physiological parameters between the Habitual MIP and the Neuromuscular Target Position, illustrating the "Hyperactivity Gap" driven by spatial discrepancy. Sources.³
5. The Great Debate: Centric Relation vs. Myocentric Occlusion
The analysis of wear patterns and mandibular retrusion inevitably intersects with one of dentistry's most enduring and contentious debates: the definition of the "ideal" jaw position. This debate frames how clinicians interpret the discrepancy found via wear pattern analysis and dictates the therapeutic approach.
5.1. The Gnathological Paradigm (Centric Relation)
Traditional Gnathology, a school of thought that has dominated restorative dentistry for decades, defines Centric Relation (CR) as a ligament-guided, bone-to-bone relationship. The classic definition (though it has evolved) considers CR as the most superior, anterior position of the condyle within the glenoid fossa, with the disc properly interposed, independent of tooth contact.¹⁰
Philosophy: The joint determines the occlusion. Treatment aims to seat the condyle in the "terminal hinge axis" and then adjust or restore the teeth to fit this specific condylar position.
Critique in Retrusion: In patients with mandibular retrusion, the gnathological CR often coincides geographically with the retruded position that is causing the airway constriction and muscle strain. Critics argue that forcing a retruded mandible back into CR - often done via "chin point guidance" or bimanual manipulation - may exacerbate the posterior displacement that the neuromuscular system is actively trying to avoid (as evidenced by the anterior wear facets).²² If the muscles are grinding the jaw forward to breathe, locking it back into CR creates a permanent conflict.
5.2. The Neuromuscular Paradigm (Myocentric Occlusion)
Neuromuscular Dentistry (NMD), pioneered by Bernard Jankelson, offers an alternative paradigm. NMD posits that the "ideal" position is determined by the muscles, not the ligaments or bones alone.⁹ The relationship of the mandible to the cranium is physiologic, not merely anatomic.
Philosophy: Myocentric Occlusion is defined as the terminal point of closure along an isotonic trajectory from the physiologic rest position.⁷ It prioritizes muscle relaxation and optimal length-tension relationships over the geometric seating of the condyle.
Role of TENS: NMD utilizes Ultra-Low Frequency (ULF) TENS (Transcutaneous Electrical Neural Stimulation) via the Myo-monitor to fatigue and relax the masticatory muscles. This specific frequency (typically 0.67 Hz) pulses the motor branches of the trigeminal (V) and facial (VII) nerves, erasing the "engram" (habitual muscle memory) of the retruded bite.¹² This allows the mandible to find its true, uncompensated rest position - the "launch pad" - without the interference of proprioceptive feedback from the teeth.
Relevance to Wear Patterns: The position found via TENS (the Myocentric position) often aligns closely with the position indicated by the Anterior Wear Facet Registration Technique. Both methods, one instrumental (TENS), one forensic (wear facets), point to a mandibular position that is more anterior and vertically open than the habitual MIP or CR.³ The wear facets are essentially the muscles' historical "vote" for the myocentric position, cast against the skeletal CR position.
5.3. Conflict and Convergence
The "war" between these philosophies ²⁴ centers on whether the reference position should be skeletal (CR) or muscular (Myocentric). In cases of mandibular retrusion, the evidence from wear patterns strongly supports the muscular perspective: the teeth are being worn down because the muscles are functioning anterior to the skeletal restriction. The wear facets demonstrate that the patient is effectively "auto-treating" their retrusion by grinding the jaw forward. Gnathology might view this forward posture as a "deviated" or "postured" slide that needs to be eliminated to return to CR. Neuromuscular dentistry views it as a physiologic necessity that needs to be supported and stabilized.
6. Neuromuscular Adaptation: Physiology and Mechanism
The term "neuromuscular adaptation" describes a sophisticated, multi-level physiological process involving the CNS, peripheral nerves, and muscle fibers. It is not merely a "habit" but a re-programming of the motor system.
6.1. The Engram and Proprioception
The central nervous system (CNS) programs muscle movements based on sensory feedback from the periodontal ligament (PDL), TMJ mechanoreceptors, and muscle spindles.⁹ This programmed pattern is called a muscle engram.¹⁴
The Avoidance Pattern: In a patient with retrusion, the teeth often interfere with the optimal path of closure. If the mandible were to close along a relaxed arc, the incisors might clash. To prevent this damage, the CNS creates an "avoidance pattern" or "accommodation." It programs the lateral pterygoid muscles to steer the mandible around the interferences and slide it back into the maximal fit (MIP).
Pathological Learning: Over time, this pathological accommodation becomes the established engram. The muscles "learn" to hold the jaw in a strained, retruded position to avoid the noxious stimuli of clashing teeth.¹⁵ The wear facets appear when this engram breaks down, typically during sleep, when cortical inhibition lowers, and the "primitive" or "vital" drive (e.g., for airway) overrides the learned avoidance pattern, causing the teeth to crash into each other.
6.2. Isotonic vs. Isometric Contraction
Normal function utilizes isotonic contraction (muscle shortens, tension remains constant) to move the mandible. The adaptive holding of a retruded mandible requires isometric contraction (muscle length remains constant, tension increases).¹² Isometric holds are metabolically devastating. They impede blood flow through the muscle belly, leading to hypoxia and the accumulation of algogenic (pain-inducing) substances like bradykinin, substance P, and prostaglandins. This physiological state explains why the "spatial discrepancy" leads to pain: the metabolic cost of maintaining the discrepancy via isometric contraction is biologically unsustainable.
6.3. Remodeling of the TMJ
Adaptation is not limited to muscles. The TMJ itself undergoes remodeling. In retrusion, the constant posterior pressure on the condyle can stimulate adaptive changes in the bone and cartilage. The condyle may flatten, and the articular eminence may remodel to accommodate the functional demands.²⁶ This is often seen as osteophytes on the condyle or flattening of the condyle or eminence. However, when the "adaptation demands exceed individuals' biological capacity," this remodeling shifts from physiologic (adaptive) to pathologic (degenerative), resulting in osteoarthritis or degenerative joint disease (DJD).²⁶ The anterior wear facets are often a warning sign that the system is functioning at the limit of its adaptive capacity and is transitioning toward breakdown.
7. Clinical Protocol: Diagnostic and Therapeutic Integration
Based on the synthesis of the "Tooth wear pattern analysis" document and the supporting neuromuscular literature, a comprehensive clinical protocol emerges for the management of mandibular retrusion. This protocol shifts the focus from "fitting teeth" to "optimizing function."
7.1. Diagnostic Phase: The Forensic Exam
The diagnostic phase is critical for identifying the discrepancy before any irreversible treatment is performed.
Wear Pattern Analysis: The clinician must inspect the incisal edges of the anterior teeth. If wear is present, request the patient to "push your jaw forward and see if you can match these wear spots." Observe the A-P (Anterior-Posterior) shift required to lock the facets.
2. Quantification: Measure the horizontal (overjet) and vertical gap in this facet-aligned position compared to the habitual MIP. A discrepancy greater than 2mm suggests significant neuromuscular displacement.¹⁶
3. Instrumentation (Recommended):
• Surface EMG: Measure resting activity of the temporalis and masseter. High resting activity (e.g., > 2.0 microvolts) confirms muscle hyperactivity and the lack of a true rest position.¹⁹
• TENS (Myo-monitor): Use ULF-TENS to relax the musculature for 45-60 minutes. This "erases" the engram.
• Kinesiography (CMS): Track the path of closure. A "zig-zag" or deviated path indicates avoidance patterns. Ideally, the TENS-induced trajectory should align with the position suggested by the wear facets.⁴
7.2. Therapeutic Phase: Establishing the New Position
The therapeutic goal is to eliminate the discrepancy - to make the "habitual" bite coincide with the "neuromuscular" target.
Orthotic Therapy: Treatment should almost always begin with a reversible phase. A removable mandibular orthotic (splint) is fabricated at the neuromuscular position (often approximating the wear facet alignment). This appliance provides a new "synthetic occlusal table" that allows the mandible to close into the optimal position without tooth interference.²⁸
Test Drive and Healing: The orthotic is worn 22/24 hours per day (except for cleaning and eating). This "test drives" the new position. It allows the muscles to heal, inflammation in the TMJ to subside, and the metabolic waste products to flush out. Success is measured by the resolution of symptoms (pain relief, increased range of motion) and the stability of objective metrics (low EMG numbers).³⁰
Reversible vs. Irreversible: Only after symptoms resolve and the position is verified (stable EMG, stable posture) should irreversible restorative work begin.
Restorative Reconstruction: When restoring, the new occlusion is built to the Myocentric position defined by the orthotic. This often requires increasing the Vertical Dimension of Occlusion (VDO) to accommodate the anterior shift and relax the muscles. As noted in the Shadman et al. clinical report, full mouth reconstruction at this new VDO is often necessary to permanently stabilize the patient.³
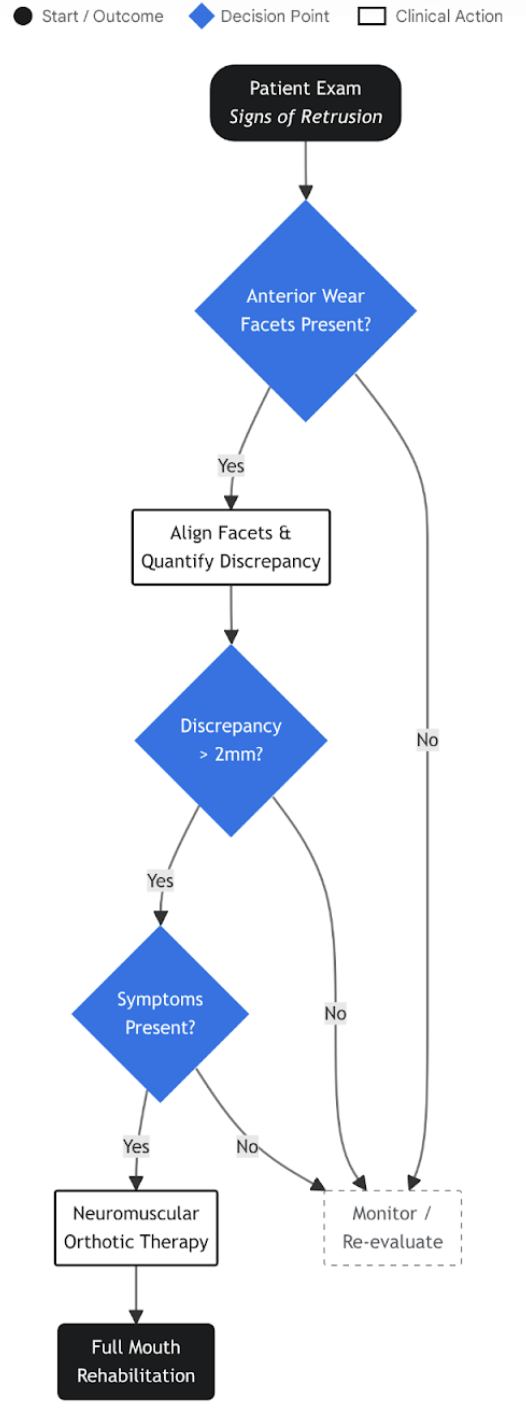
Clinical Decision Algorithm: Managing Mandibular Retrusion via Wear Analysis
A stepwise clinical protocol for utilizing wear pattern analysis in diagnosis. The workflow integrates visual inspection, facet alignment, and quantification of discrepancy to determine the necessity for neuromuscular Orthotic intervention versus simple monitoring.
Data sources: Tooth Wear Analysis PDF, PS Dental Care, Dentistry Today
8. Broader Implications: Posture and Systemic Health
The implications of this research extend far beyond the oral cavity. The "ripple effects" of mandibular retrusion and neuromuscular adaptation touch upon total body health, validating the concept of the stomatognathic system as a central pillar of postural and respiratory integrity.
8.1. Descending Chains and Cervical Posture
The stomatognathic system is mechanically and neurologically linked to the cervical spine via the hyoid bone, the infrahyoid muscles, and the deep cervical fascia. Mandibular retrusion often forces a Forward Head Posture (FHP). As the airway is compromised by the retruded tongue, the patient reflexively extends the head forward to stretch the neck and open the pharyngeal space.³¹
The Chain Reaction: FHP alters the center of gravity of the head (which weighs 10-12 lbs). To compensate, the posterior cervical muscles (trapezius, splenius capitis) must contract isometrically to prevent the head from falling forward. This leads to chronic neck pain, tension headaches, and even changes in lumbar curvature (lordosis) as the spine attempts to rebalance.³¹
Correction: Correcting the mandibular position (moving it anteriorly to the neuromuscular target indicated by wear facets) has been shown to improve cervical posture. Studies indicate that a myocentric position facilitates a return to a neutral head posture, reducing the load on the cervical spine.²⁵
8.2. Airway and Sleep Apnea
Perhaps the most critical implication relates to Obstructive Sleep Apnea (OSA). The anterior wear patterns discussed in this report essentially mimic the position of a Mandibular Advancement Device (MAD), the standard dental treatment for sleep apnea. The patient is, in effect, subconsciously treating their own airway obstruction by grinding the jaw forward at night.
The Danger of Retrusion: If a clinician ignores these wear patterns and restores the patient back to a retruded CR position (pushing the jaw back), they could inadvertently exacerbate sleep apnea or Upper Airway Resistance Syndrome (UARS) by reducing the airway volume.⁵
The Wear Facet as a Sign: Severe anterior wear facets should be considered a "red flag" for sleep disordered breathing. The wear pattern analysis thus becomes a screening tool not just for TMJ pathology, but for life-threatening respiratory disorders.
9. Conclusion
The analysis of anterior wear facets in patients with mandibular retrusion offers a profound shift in diagnostic perspective for the dental practitioner. These dental modifications are not merely pathological signs of structure loss to be patched with composite or porcelain; they are functional blueprints of neuromuscular intent. They reveal a persistent, physiological drive by the masticatory system to correct the compromised skeletal position imposed by mandibular retrusion.
The discrepancy between the habitual bite (MIP) and the position dictated by these wear facets is a quantifiable metric of neuromuscular strain. It represents the "Hyperactivity Gap" that drives chronic pain, joint degeneration, and muscle fatigue. By recognizing this discrepancy, clinicians can move beyond the static limitations of traditional Gnathology and embrace a dynamic, physiologic approach. Treatment directed at aligning the occlusion with this neuromuscular target - using the "launch pad" of physiologic rest as the reference - offers the potential to resolve chronic pain, restore efficient function, and harmonize the stomatognathic system with the broader demands of airway patency and cervical posture. The wear facets, in essence, point the way to the position where the body is most at ease.
References
Functional Adaptations in the Temporomandibular Joint - University of Michigan, accessed February 16, 2026, https://media.dent.umich.edu/labs/mcnamara/files/Functional%20adaptations%20in%20the%20temporomandibular%20joint.pdf
Occlusion and Temporomandibular Disorders: A Scoping Review - PMC, accessed February 16, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC12112774/
Tooth wear pattern analysis.pdf
Neuromuscular Evaluation in Orthodontic–Surgical Treatment: A Comparison Between Monomaxillary and Bimaxillary Surgery - MDPI, accessed February 16, 2026, https://www.mdpi.com/2306-5354/13/1/123
The impact of mouth breathing on dentofacial development: A concise review - Frontiers, accessed February 16, 2026, https://www.frontiersin.org/journals/public-health/articles/10.3389/fpubh.2022.929165/full
Oropharyngeal Growth and Skeletal Malformations - Academy of Orofacial Myofunctional Therapy, accessed February 16, 2026, https://aomtinfo.org/wp-content/uploads/2017/09/2016-Chapter-143-Oropharyngeal-Growth-and-Malformations-PPSM-6e-1.pdf
MYOCENTRIC - Occlusion Connections, accessed February 16, 2026, https://occlusionconnections.com/neuromuscular-dentistry/myocentric/
Strength improvements through occlusal splints? The effects of different lower jaw positions on maximal isometric force production and performance in different jumping types | PLOS One, accessed February 16, 2026, https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0193540
LITERATURE REVIEW OF - ICCMO, accessed February 16, 2026, https://iccmo.org/Content/Files/ICCMO-Literature-Review.pdf
THE GNATHOLOGICAL APPROACH versus THE NEUROMUSCULAR APPROACH - Occlusion Connections, accessed February 16, 2026, https://occlusionconnections.com/occlusion/the-gnathological-approach-versus-the-neuromuscular-approach/
RETRACTED ARTICLE: Treatment of temporomandibular joint internal derangement using MESNA injection - PMC, accessed February 16, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11299281/
Clinical Studies - LVI Global, accessed February 16, 2026, https://www.lviglobal.com/2015/06/23/clinical-studies/
Technical note: Occlusal fingerprint analysis: Quantification of tooth wear pattern - UG Dental, accessed February 16, 2026, https://ug-dental.de/wp-content/uploads/2017/07/occlusal-Fingerprint-4-1.pdf
Comparative Evaluation of Occlusion before and after Soft Tissue Mobilization in Patients with Temporomandibular Disorder - Myofascial Pain with Referral - PMC, accessed February 16, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC8296451/
Use of Tens in the Diagnosis of Functional Mandibular Lateral Deviation - MDPI, accessed February 16, 2026, https://www.mdpi.com/2076-3417/13/24/13258
Mandibular rest position and electrical activity of the masticatory muscles - ResearchGate, accessed February 16, 2026, https://www.researchgate.net/publication/13982946_Mandibular_rest_position_and_electrical_activity_of_the_masticatory_muscles
The effect of neuromuscular training on an edentulous patient with unstable mandibular position and uncoordinated mandibular movements: a clinical report - PMC, accessed February 16, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC11998229/
The adaptive response of jaw muscles to varying functional demands - Oxford Academic, accessed February 16, 2026, https://academic.oup.com/ejo/article/31/6/596/465295
Mandibular rest position and electrical activity of the masticatory muscles - PubMed, accessed February 16, 2026, https://pubmed.ncbi.nlm.nih.gov/9237146/
Tooth Wear: Prevention, Treatment, and Monitoring Using the T-Scan/BioEMG Synchronization Module - ResearchGate, accessed February 16, 2026, https://www.researchgate.net/publication/382426770_Tooth_Wear_Prevention_Treatment_and_Monitoring_Using_the_T-ScanBioEMG_Synchronization_Module
CENTRIC RELATION BETWEEN CHIMERA AND REALITY- A NARRATIVE REVIEW, accessed February 16, 2026, http://rjor.ro/wp-content/uploads/2023/12/CENTRIC-RELATION-BETWEEN-CHIMERA-AND-REALITY-.pdf
How Effective Is the Neuromuscular Occlusion Approach in diagnosing and treating TMD?, accessed February 16, 2026, https://oasisdiscussions.ca/2013/03/11/tmd/
Current concepts of trauma from occlusion - A review - ResearchGate, accessed February 16, 2026, https://www.researchgate.net/publication/333142449_Current_concepts_of_trauma_from_occlusion_-_A_review
Politics vs. Science - ICCMO, accessed February 16, 2026, https://iccmo.org/neuromuscular-controversies-politics-v-science
Analysis of the postural stability in individuals with or without signs and symptoms of temporomandibular disorder - SciELO, accessed February 16, 2026, https://www.scielo.br/j/bor/a/vmH9jTftWLq33R4W8Gx8mcq/
Exploring the Complexities of Temporomandibular Joint Function and Dysfunction: A Contemporary Review, accessed February 16, 2026, https://www.scielo.sa.cr/scielo.php?script=sci_arttext&pid=S2215-34112024000300079
Cone-Beam CT-Based Analysis of Temporomandibular Joint Osseous Changes in Orthognathic Surgery Patients: A Retrospective Cross-Sectional Study - PMC, accessed February 16, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC12785262/
Measurable Changes in TMD Patients' Cervical-Mandibular Posture following Myofunctional Therapy, Frenectomy, and Neuromuscular Orthotic - Advanced Dental Technologies & Techniques, accessed February 16, 2026, https://adtt.scholasticahq.com/article/138294-measurable-changes-in-tmd-patients-cervical-mandibular-posture-following-myofunctional-therapy-frenectomy-and-neuromuscular-orthotic
Functional-Cosmetic Dentistry: A Full-Mouth Smile Makeover, Part 2, accessed February 16, 2026, https://www.dentistrytoday.com/sp-1107584113/
The Role of Neuromuscular Dentistry in Enhancing Jaw Alignment and Comfort, accessed February 16, 2026, https://www.psdentalcare.co.uk/post/the-role-of-neuromuscular-dentistry-in-enhancing-jaw-alignment-and-comfort
Neuromuscular dentistry: Occlusal diseases and posture - PMC - NIH, accessed February 16, 2026, https://pmc.ncbi.nlm.nih.gov/articles/PMC3941922/
Perspectives on Pathological Crosstalk between Malocclusion and Multi-organ Systems: The Hidden Face of an Iceberg - Aging and disease, accessed February 16, 2026, https://www.aginganddisease.org/EN/10.14336/AD.2025.1377