

2025-09-30
The Bruxism Conundrum: A Deep-Dive Analysis of its Long-TermImpact on Dental Implant Success
By Dr. Agatha Bis
Section 1: Introduction: The Biomechanical Challenge of Parafunction on Osseointegrated Implants
1.1 The Paradox of Modern Implant Dentistry
Modern implant dentistry stands as one of the most predictable and successful disciplines in clinical practice, with long-term studies consistently reporting survival rates of 95% or higher over periods of 8 to 10 years.¹ This remarkable success has positioned osseointegrated implants as the standard of care for replacing missing teeth. However, this success is predicated on a state of biomechanical equilibrium, a state that is profoundly disrupted by the presence of parafunction and bruxism. Bruxism, a repetitive and often forceful jaw-muscle activity, introduces non- physiological loads that challenge the very foundation of osseointegration.⁴ This creates a clinical paradox: a highly predictable treatment modality confronting a highly destructive patient-specific condition. Consequently, parafunction and bruxism are no longer viewed as absolute contraindications for implant therapy but are now widely recognized as a significant risk factor that necessitates a paradigm shift in diagnosis, treatment planning, and long-term management.⁷ The successful long-term care of a parafunction or bruxing patient with dental implants depends entirely on the clinician's ability to identify, mitigate, and manage these destructive forces.
1.2 The Critical Absence of the Periodontal Ligament (PDL)
The fundamental vulnerability of a dental implant to parafunctional forces stems from a critical anatomical difference between it and a natural tooth: the absence of a periodontal ligament (PDL). In the natural dentition, the PDL is a sophisticated viscoelastic structure that serves two vital functions. First, it acts as a natural shock absorber, dissipating occlusal forces and dampening their transmission to the alveolar bone. Second, it is rich in mechanoreceptors that provide precise proprioceptive feedback to the central nervous system, creating a sensitive regulatory loop that modulates masticatory muscle activity and protects the tooth from excessive loading.¹⁰
A dental implant, by contrast, is functionally ankylosed. It achieves stability through osseointegration, a direct structural and functional connection between living bone and the implant surface.¹² This rigid interface lacks the cushioning and sensory properties of the PDL.¹³ As a result, occlusal loads are transferred directly and unbuffered to the bone-implant interface and the prosthetic components. The proprioceptive feedback loop is dramatically diminished, with some studies suggesting an eight-fold reduction in tactile sensitivity compared to a natural tooth.¹¹ This creates a uniquely perilous situation. A patient with bruxism, an involuntary and often subconscious muscle activity, can generate and sustain pathologic forces on an implant-supported restoration without the normal biological feedback that would signal the central nervous system to cease or moderate the activity.⁸ The problem, therefore, is not merely one of excessive force, but of uncontrolled and unperceived excessive force. While normal mastication involves brief, intermittent contacts totalling approximately 9 to 17 minutes per day, parafunction and bruxism can involve prolonged periods of intense loading, leading to material fatigue and biological complications that would not occur under physiologic conditions.¹¹
1.3 Defining the Threat: Bruxism and Occlusal Overload
To effectively manage the risk, a precise understanding of the terminology is essential. Based on an international expert consensus, bruxism in mainstream literature is defined as a repetitive jaw-muscle activity characterized by clenching or grinding of the teeth and/or by bracing or thrusting of the mandible.¹⁶ It is crucial to distinguish between its two manifestations:
Sleep Bruxism (SB): A masticatory muscle activity during sleep that is characterized as rhythmic (phasic) or non-rhythmic (tonic) and is not a movement disorder or a sleep disorder in otherwise healthy individuals.¹⁸
Awake Bruxism (AB): A masticatory muscle activity during wakefulness characterized by repetitive or sustained tooth contact and/or by bracing or thrusting of the mandible.¹⁸
The prevalence of bruxism is significant, with studies reporting rates of approximately 13% for SB and up to 31% for AB in adult populations.¹⁶ While historically associated with malocclusion, the etiology is now understood to be multifactorial, with central factors like stress, anxiety, sleep disorders, and the use of substances like alcohol, caffeine, and tobacco being more consistently implicated.¹⁹
Bruxism leads to occlusal overload, which is defined as any occlusal force that results in damage to the stomatognathic structures, including the implant fixture, prosthetic components, and the supporting peri-implant bone.¹² The damaging potential of these forces is a function of several variables, including magnitude, duration, frequency, and, critically, direction.1 The lateral, non-axial forces generated during grinding excursions are particularly destructive to the implant system, which is engineered primarily to withstand forces along its long axis.¹
Section 2: Diagnostic Imperatives: Identifying the Bruxer and Signs of Occlusal Overload
2.1 A Multi-faceted Diagnostic Approach
The early identification of parafunction and bruxism is the first and most critical step in mitigating its long-term impact on dental implants. Since definitive diagnosis with polysomnography is impractical for routine dental screening, clinicians rely on a graded diagnostic framework to establish the likelihood of the condition.¹⁶ This approach categorizes bruxism as:
Possible Bruxism: Based on patient self-report via questionnaires or interviews.
Probable Bruxism: Based on a positive self-report combined with positive findings from a clinical examination.
Definitive Bruxism: Based on positive self-report, positive clinical findings, and confirmation via instrumental assessment (e.g., electromyography or polysomnography).
For the purposes of clinical risk assessment in implant dentistry, identifying "probable bruxism" is the actionable goal.¹⁶ This requires a comprehensive evaluation that includes a detailed patient history, probing for factors associated with bruxism such as high stress levels, anxiety, sleep disturbances, and the use of alcohol, caffeine, tobacco, or certain psychotropic medications like antidepressants.¹⁹
2.2 Early Warning Signs: Clinical Indicators of Parafunction and Overload
A thorough clinical examination can reveal a constellation of signs that point toward active parafunction and occlusal overload. These indicators are often subtle in their early stages and must be actively sought by the clinician.
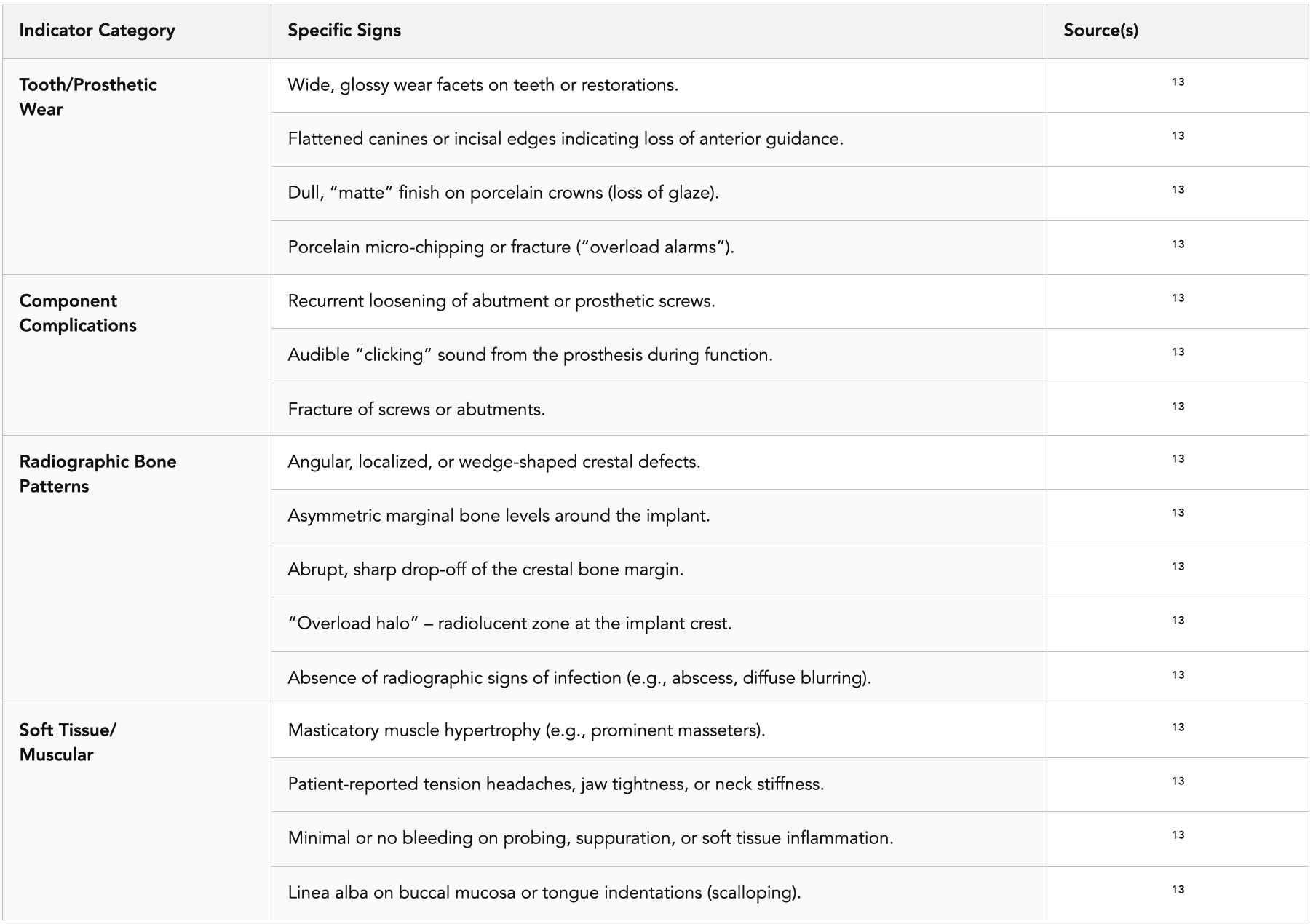
Wear Patterns and Tooth Structure: The most obvious signs are found on the teeth themselves. Clinicians should look for wide, glossy wear facets on the occlusal and incisal surfaces of remaining natural teeth or existing restorations. A simple chair-side test involves drying the tooth and observing it with oblique light; a facet from parafunction will flash like glass.¹³ Flattened canines and incisal edges are particularly significant, as they indicate the loss of anterior guidance, a protective mechanism that discludes posterior teeth during excursions. When this guidance is lost, posterior implants are forced to bear damaging lateral loads.¹³
Porcelain and Crown Damage: Prosthetic restorations serve as sensitive barometers of overload. An untouched porcelain glaze has a distinct, mirror-like shine. After months of bruxing, this glaze can be stripped away, leaving a dull, chalky, or "matte" finish. This de-glazed surface has significantly higher friction, accelerating wear on both the restoration and the opposing dentition. A useful test is to gently run an explorer tip sideways across the crown; a glazed surface feels slick, while a de-glazed one will "grab" the explorer.¹³ More advanced signs include porcelain micro-chipping or fractures. These are critical "overload alarms," indicating that tensile and shear forces have exceeded the ceramic's material strength, which is robust under compression (≈1,200 MPa) but weak under tension (≈30−50 MPa).¹³
Component Complications: The internal components of the implant system often show the first signs of mechanical distress. Recurrent loosening of the abutment or prosthetic screw is a cardinal sign of overload. This may be accompanied by an audible "clicking" sound during function, which should prompt immediate investigation.¹³ This loosening is a direct precursor to the more severe complication of screw fracture.
Muscle and Soft Tissue Signs: The effects of parafunction extend beyond the dentition. Chronic hyperactivity can lead to hypertrophy of the masticatory muscles, particularly the masseter. Patients may report symptoms such as tension-type headaches, unexplained neck stiffness, or a feeling of a "tight jaw".¹³ Intraorally, a linea alba (a white line on the buccal mucosa at the level of the occlusal plane) or indentations on the tongue can be indicative of clenching or bracing habits.¹⁷ Look for tongue or cheek scalloping, which is a sign of parafunction rather than a normal finding.
2.3 Radiographic Hallmarks of Mechanical Stress
Radiographic evaluation is paramount, as it can reveal the impact of overload on the supporting bone and help differentiate mechanical stress from infection-driven bone loss.
The Signature Defect: The pathognomonic radiographic sign of occlusal overload is an angular, localized, wedge-shaped crestal bone defect at the neck of the implant.¹³ This defect's geometry is aligned with the axis of the damaging load. It stands in stark contrast to the broader, saucer-shaped, or crater-like circumferential resorption typically associated with bacterial peri- implantitis.¹³
Other Radiographic Clues: Other signs reinforce the diagnosis of mechanical stress. These include asymmetric marginal bone levels around the implant, an abrupt and sharply demarcated angular drop-off of the crestal bone margin, and bone loss that appears to respect the pitch of the implant threads.¹³ In some cases, an "overload halo," a subtle radiolucent zone around the implant crest, may be visible, representing metabolic stress in the bone from repeated overload.¹³ A critical diagnostic feature is that these radiographic changes often occur in the clinical absence of soft tissue inflammation and in the radiographic absence of signs of infection, such as diffuse bone blurring or abscess formation.¹³
To aid clinicians in systematically identifying these varied signs, the following diagnostic checklist is proposed.
Table 1: A Clinical and Radiographic Checklist for Identifying Occlusal Overload on Dental Implants.
Section 3: The Central Controversy: Is Occlusal Overload a Cause or a Co-Factor for Crestal Bone Loss?
3.1 Dissecting the Debate: The Two Competing Hypotheses
Once bone loss is detected around an implant, the clinician faces a critical diagnostic crossroads. Is the bone loss a direct result of excessive mechanical force, or is it driven by a bacterial infection? The answer to this question dictates the entire treatment approach. This diagnostic challenge lies at the heart of a long-standing controversy in implant dentistry, framed by two competing hypotheses.¹¹
Hypothesis 1: Overload as a Primary Etiologic Factor. This hypothesis assumes that excessive occlusal forces, even in a sterile, non-inflamed environment, are sufficient to cause crestal bone loss. The proposed mechanism involves the creation of micro-fractures in the bone at the implant interface. When the rate of micro-damage from pathologic loading exceeds the bone's capacity for repair, a net resorption of bone occurs, leading to loss of osseointegration and eventual implant failure.¹² Proponents of this view argue that the rigid, ankylosed nature of the implant makes the surrounding bone uniquely susceptible to this type of direct mechanical damage.
Hypothesis 2: Overload as a Co-destructive Factor. Drawing a direct parallel from the well-established "co-destruction theory" in periodontology, this hypothesis argues that occlusal overload alone does not initiate bone loss around a healthy, non-inflamed implant. Instead, it acts as an accelerating or exacerbating factor. According to this model, a bacterial biofilm must first be present to initiate an inflammatory response in the peri-implant tissues (peri- mucositis). If this inflammation is left untreated and progresses to peri- implantitis, the presence of occlusal overload will then significantly amplify the rate and severity of the infection-driven bone destruction.²² In this view, inflammation is the trigger, and overload is the amplifier.
3.2 Synthesizing Conflicting Evidence
The persistence of this debate is fuelled by a body of scientific literature that is fraught with conflicting results and methodological challenges.
• Evidence from Animal Studies: The evidence from animal models is particularly contradictory. Some early studies in monkeys and other animals suggested that applying excessive loads to implants could, by itself, lead to significant bone loss and complete loss of osseointegration.¹¹ However, a larger body of more recent and well-controlled animal studies has failed to replicate these findings. These studies, conducted primarily in dogs and monkeys with meticulous plaque control, have shown that applying excessive occlusal loads in a non-inflamed environment does not cause marginal bone loss and, in some cases, can even be anabolic, leading to increased bone density and bone-to-implant contact.¹⁴ The same studies often demonstrate that when plaque-induced inflammation is present, the addition of overload dramatically worsens bone loss, supporting the co- destruction hypothesis.²⁷ The discrepancies among these studies are likely due to significant confounding variables, including differences in animal models, the magnitude and direction of applied forces, the duration of loading, and the effectiveness of oral hygiene protocols.¹¹
Evidence from Human Clinical Studies: The ethical impossibility of conducting controlled trials that intentionally overload implants in humans means that the clinical evidence is entirely indirect, derived from retrospective and observational studies.¹¹ These studies are inherently susceptible to confounding factors and bias. Systematic reviews of this clinical literature reflect the uncertainty. Some reviews have found a positive correlation between clinical signs of overload (such as wear facets or non-ideal prosthetic design) and crestal bone loss.²⁶ For instance, one systematic review found that four out of seven included studies reported a positive correlation between overload and crestal bone loss.³⁰ Conversely, other reviews have concluded there is little unbiased evidence to support a direct cause-and-effect relationship.²⁷ A critical finding across multiple reviews is that the included studies almost universally suffer from a moderate to serious risk of bias, primarily due to retrospective designs and the use of non-quantifiable, subjective methods for assessing overload.²⁶
This ongoing debate may be partially reconciled by moving beyond a simple binary choice. The clinical reality is likely more nuanced. The implant system, comprising the fixture, the bone, the abutment, the screw, and the crown, is a single biomechanical unit. Parafunctional overload is a stressor that attacks this entire system. The first component to fail is likely the one that represents the "weakest link" for that individual patient. For instance, a patient with excellent oral hygiene and dense, high-quality bone may present with repeated mechanical failures, including porcelain chipping, screw loosening, or even screw fracture, as the prosthetic components are the weakest link.¹³ This aligns with systematic reviews suggesting bruxism is a more clearly established risk factor for mechanical complications than for biological ones.¹⁵ In contrast, a patient with poorer bone quality (e.g., Type 4 bone in the posterior maxilla) or pre-existing low-grade inflammation may present with crestal bone loss as the first sign of trouble, as the bone-implant interface is the weakest link, and the overload accelerates its breakdown.²⁵ This perspective suggests that overload and peri-implantitis are not always mutually exclusive diagnoses but can be interacting pathologies, and the clinical presentation depends on a patient's unique host factors.
3.3 The Critical Distinction from Peri-implantitis
Regardless of the academic debate, the clinician must make a practical decision at the chair-side. Misdiagnosing overload as infection leads to ineffective treatment (e.g., surgical debridement that fails to address the underlying mechanical cause), while misdiagnosing infection as overload is equally futile (e.g., an occlusal adjustment that fails to address the bacterial etiology). Therefore, a clear differential diagnosis is essential.
Etiology: The fundamental difference is mechanical versus biological. Overload is caused by excessive, misdirected, or prolonged forces, often from parafunction. Peri-implantitis is caused by a pathogenic bacterial biofilm.¹³
Clinical Presentation: Overload is often clinically "silent." The peri-implant tissues may appear healthy, with firm, pink mucosa and little to no bleeding on probing or suppuration (pus).¹³ The primary clinical findings are mechanical: wear facets, chipped porcelain, or loose components.¹³ In contrast, peri- implantitis presents with the classic signs of inflammation: red, swollen, and edematous mucosa, significant bleeding on gentle probing, and often suppuration.¹³
Radiographic Appearance: As previously described, the radiographic signatures are distinct. Overload typically produces sharp, angular, or wedge- shaped crestal defects confined to the implant neck. Peri-implantitis produces more diffuse, saucer-shaped or crater-like defects that are often circumferential around the implant.¹³
The following table summarizes the key features to aid in this critical differential diagnosis.
Table 2: Differential Diagnosis of Bone Loss Around Dental Implants: Occlusal Overload vs. Peri-implantitis.

Section 4: Quantifying the Risk: A Review of Long-Term Clinical Evidence
4.1 The Weight of Evidence: Findings from Systematic Reviews & Meta-Analyses
While the precise mechanism of overload-induced bone loss remains debated, the clinical association between parafunction and bruxism and adverse implant outcomes is strongly supported by high-level evidence. Multiple systematic reviews and meta- analyses, which pool data from numerous individual studies, consistently identify parafunction and bruxism as a significant risk factor for both mechanical complications and outright implant failure.
The quantitative findings from these reviews are compelling. One meta-analysis reported that bruxism was associated with an odds ratio (OR) of 4.68 for mechanical issues and implant loss, meaning patients with bruxism had nearly five times the odds of experiencing these complications compared to non-bruxers.¹⁶ Another meta-analysis focusing on prosthesis failures found a remarkably similar OR of 4.72 in bruxers.³⁴ A more recent systematic review and meta-analysis from 2024 calculated a significant risk of implant failure in probable bruxers, with an OR of 2.189.²³ Other analyses have reported hazard ratios of 3.396 and odds ratios of 2.71 for implant failure in bruxers.¹¹ While the exact figures vary slightly depending on the studies included and the specific outcomes measured, the consistent direction and statistical significance of these findings across independent, high-level reviews provide a powerful signal. They establish a clear clinical association that cannot be ignored in treatment planning and patient management.
Table 3: Summary of High-Level Evidence from Key Meta-Analyses and Reviews on Bruxism and Implant Failure.

4.2 The Long-Term Prognosis: Data from Longitudinal Studies
Longitudinal studies, which track patients over many years, provide a real-world picture of how this statistical risk translates into clinical outcomes over time. The data clearly show a progressive degradation of implant survival rates in patients with unmanaged bruxism.
A 5-year retrospective study cited in a 2019 review painted a stark picture of declining survival: the rate for implants in bruxers was 90% after 1 year, dropping to 87% after 2 years, 85% after 3 years, 75% after 4 years, and just 72% after 5 years.¹¹ This demonstrates a significant and continuous attrition rate over the medium term.
A long-term study with a 15-year follow-up provided even more granular data. It found that when bruxism was the only identifiable risk factor, the implant failure rate was 14.55%, corresponding to a success rate of 85.45% over the study period.³⁷ This is substantially lower than the 95-98% success rates typically reported for the general population. The study also highlighted the synergistic effect of multiple risk factors; when bruxism was combined with other factors like smoking, diabetes, and a history of periodontal disease, the failure rate soared to a staggering 40%.³⁷ Another large retrospective study involving over 3,500 implants found that the failure rate in diagnosed bruxers was 13.0%, compared to just 4.6% in non-bruxers; a nearly three- fold increase.³⁵ These figures provide tangible evidence of the long-term jeopardy that bruxism poses to implant restorations.
4.3 The Cascade of Failure: A Biomechanical Sequence
The elevated failure rates observed in bruxers are often the culmination of a predictable sequence of mechanical complications. This cascade of failure begins with subtle signs and progresses to catastrophic events if left unmanaged. Understanding this sequence is crucial for early intervention.
Stage 1: Screw Loosening. This is frequently the first detectable sign of biomechanical distress. The repetitive, off-axis lateral forces generated during parafunction and bruxism can overcome the clamping force (preload) that holds the abutment to the implant. This leads to microscopic movements at the implant-abutment interface, which, over thousands of cycles, results in a progressive loss of torque and eventual screw loosening.¹³ A lack of passive fit in the prosthesis or improper initial torquing can exacerbate this issue.¹³
Stage 2: Prosthetic Chipping and Fracture. The next stage often involves damage to the restorative material itself. As noted, ceramics like porcelain are brittle and have low tensile and shear strength.¹³ The lateral grinding motions of bruxism generate precisely these types of damaging shear stresses. This initially manifests as chipping of the veneering porcelain on a metal-ceramic or zirconia-based crown. A smooth, clean fracture of the ceramic is a classic sign of lateral overload.¹³
Stage 3: Screw Fracture. If screw loosening is not identified and corrected, the component is subjected to continued cyclic loading in a non-stable state. This leads to metal fatigue, where microscopic cracks initiate and propagate through the screw material until it ultimately fractures. The fracture of an abutment or prosthetic screw is a clear indication that the system has been under severe, prolonged overload.¹³
Stage 4: Implant Body Fracture. This is the most severe and catastrophic mechanical complication. The fracture of the implant fixture itself is an extreme event that typically occurs only after earlier warning signs, namely screw loosening and/or fracture, have been missed or ignored.¹³ Continued parafunctional loading on a compromised prosthetic connection transfers immense stress directly to the implant body, which can eventually lead to fatigue fracture, often at the level of the first thread or the implant platform.¹³ This represents a total and often unsalvageable failure of the implant system.
Section 5: A Framework for Proactive Clinical Management and Risk Mitigation
Given the substantial evidence linking bruxism to long-term complications, a reactive, "wait-and-see" approach is inadequate. Successful management requires a proactive and systematic framework that integrates risk assessment, specialized prosthetic design, and protective appliance therapy from the outset. The goal is not simply to replace a tooth, but to engineer a restoration that can withstand a hostile biomechanical environment. This approach is not an optional add-on but a fundamental component of the standard of care for this high-risk patient population.
5.1 Pre-Treatment Risk Stratification
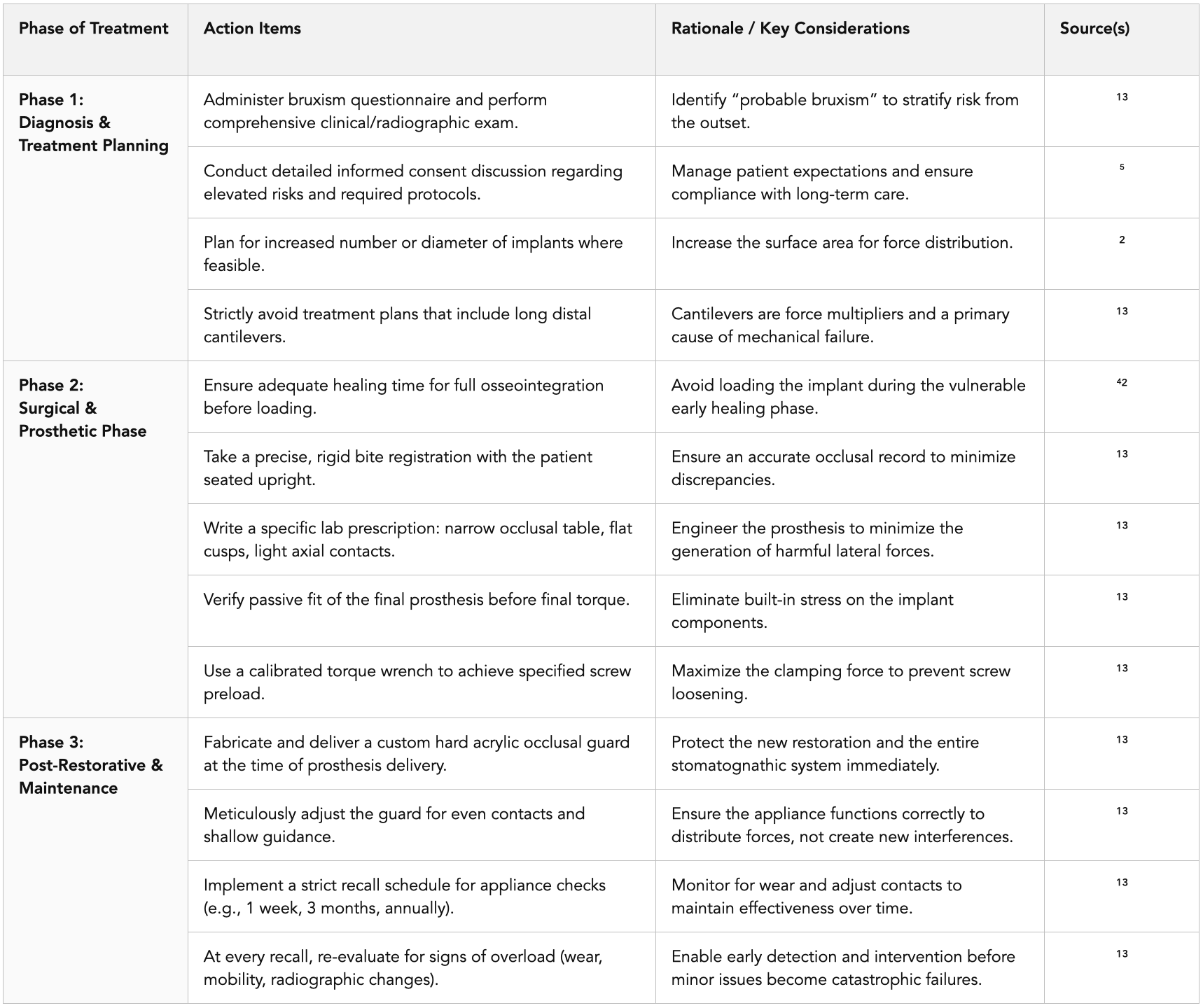
The management protocol begins at the initial consultation. Every potential implant patient should be screened for bruxism using the diagnostic methods outlined in Section 2. The identification of "probable bruxism" should immediately trigger a specific risk-mitigation pathway.⁵ This includes a thorough discussion with the patient as part of the informed consent process, clearly outlining the elevated risk of mechanical complications and implant failure, and explaining the necessity of the specialized design and maintenance protocols that will be required. This manages patient expectations and ensures their partnership in the long-term success of the treatment.
5.2 Prosthetic Design for Force Attenuation ("Occlusal Engineering")
The centrepiece of proactive management is the design of the prosthesis itself. The restoration must be intentionally engineered to dissipate and minimize the harmful forces generated by parafunction. This involves several key principles:
Occlusal Table Morphology: The occlusal (chewing) surface of the implant crown must be modified. The buccolingual width of the occlusal table should be narrowed, and the cuspal inclines should be significantly flattened or made shallow. A narrow table reduces the cantilever effect and leverage on the implant, while flat cusps minimize the generation of destructive lateral shear forces during grinding excursions. The central fossa should be widened to create a "landing pad" for the opposing cusp.¹³ Communication with the dental laboratory must be precise, with prescriptions specifying features like "Implant crown with 1.5 mm flat fossa, light axial contacts only, and no lateral contacts in excursion".¹³
Occlusal Scheme Selection: The choice of occlusal scheme must be driven by functional requirements, not aesthetic norms. The goal is to select the scheme that most effectively "bleeds off" or distributes lateral forces for that specific patient.¹³ While canine guidance is often ideal, if a patient's natural canines are worn down from years of bruxism, attempting to restore steep canine guidance on an implant-supported crown can be disastrous. In such cases, a well-balanced group function, where forces are shared among several teeth during lateral movements, may be a more protective and realistic goal.
Elimination of High-Risk Features: Certain prosthetic designs act as force multipliers and must be avoided in bruxing patients. The most significant of these is the long distal cantilever. A cantilever extension on an implant- supported bridge creates immense leverage on the terminal implant, leading to high stress concentrations, unpredictable bone loss, and a high rate of mechanical failure.¹³ While the debate over crown-to-implant ratios continues, with some evidence suggesting high ratios are not as detrimental as once thought, a conservative approach favouring shorter crown heights is still prudent in high-risk patients.¹¹
Technical Precision and Material Selection: Biomechanical stability begins with technical excellence. A completely passive fit of the prosthesis, meaning it seats without any rocking or tension, is critical to avoid built-in stress.¹³ Furthermore, achieving the correct preload on the prosthetic or abutment screw by using a calibrated torque wrench according to the manufacturer's specifications is essential. This preload creates the clamping force that resists screw loosening.¹³ Material choice also plays a role; while strong, monolithic zirconia crowns eliminate the risk of porcelain chipping, they can cause accelerated wear on the opposing natural dentition. The choice of material must be carefully weighed.
5.3 Essential Appliance Therapy
Prosthetic design alone is not sufficient. For any patient with diagnosed bruxism, a protective occlusal appliance is a non-negotiable component of long-term care. The analogy that "an unprotected implant in a bruxer is like a new phone without a case" aptly captures its importance.¹³ An appliance should be prescribed for any patient exhibiting clinical signs of wear, reporting tension headaches, or with a confirmed diagnosis of parafunction.¹³
• Device Selection: The type of appliance should be tailored to the patient's specific parafunctional pattern:
Hard Full-Arch Acrylic Guard: This is the gold standard for patients with nocturnal sleep bruxism. Fabricated from a rigid material, it provides a durable, protective barrier that distributes forces evenly across the entire arch, preventing concentrated, high-magnitude loads from impacting individual implants.¹³
Mandibular Pivot Appliance: This appliance may be indicated for severe clenchers, particularly those with full-arch "All-on-X" restorations. It is designed to help deprogram the hyperactive musculature and reduce the intensity of clenching forces.¹³ However, due to lack of anterior tooth contact while wearing the appliance, long-term or chronic use is not advised due to the possibility of anterior teeth supra-eruption, resulting in retrusion of the mandible on closing when not wearing the appliance. This could lead to further TMD challenges.
Custom Orthotic Appliance: A customized orthotic appliance, such as the BiteAlign™, is recommended for patients who wear the appliance full-time or most of the day. It provides balanced contacts across the bite while incorporating individualized guidance into the design, allowing the mandible to move freely without restriction. This creates a more physiologic jaw position, helping to reduce tension, facial pain, and headaches, while protecting teeth, restorations, and joints from uneven forces. By restoring proper function and freedom of movement, the appliance not only improves comfort and daily function but also serves as a valuable diagnostic tool that guides long-term treatment planning and supports lasting oral health.
Thin Daytime Guard: For patients who primarily exhibit awake bruxism, often associated with daytime stress or concentration, a thin, less obtrusive guard can be worn. This serves both to protect the restorations and to act as a biofeedback mechanism, helping the patient become more aware of and consciously control the habit.¹³
• Fit and Follow-Up Protocol: The fabrication of an occlusal guard is not a one-time procedure. Its effectiveness depends on a meticulous fit and diligent long-term maintenance. The appliance must be carefully adjusted at delivery to ensure even, simultaneous contacts in optimal mandible position (key to reducing symptoms), and smooth, shallow guidance in excursions. A strict follow-up protocol is essential to monitor its effectiveness and adjust for any changes in the occlusion. This should include re-evaluating the contacts at 1 week, 3 months, and then at least annually thereafter.¹³
The following table provides a structured workflow for implementing this comprehensive management strategy.
Table 4: A Clinical Protocol for Managing the Bruxer Implant Patient.
Section 6: Conclusion: Navigating Uncertainty with Evidence-Based Precaution
6.1 Summary of Key Findings
The relationship between bruxism and the long-term prognosis of dental implants is a complex interplay of biomechanics, material science, and host biology. This analysis has established several key conclusions grounded in the available evidence. First, while the precise role of occlusal overload as a primary cause of crestal bone loss remains a subject of legitimate scientific debate, the clinical evidence linking bruxism to significantly higher rates of mechanical complications and overall implant failure is robust, consistent, and quantitatively supported by numerous systematic reviews and meta-analyses.¹⁶ The odds of failure or complications are several times higher in patients with bruxism. Second, the absence of the periodontal ligament's protective mechanisms renders the implant system uniquely vulnerable to the unperceived and prolonged forces of parafunction. Third, occlusal overload manifests with a distinct set of clinical and radiographic signs, such as screw loosening, porcelain fracture, and angular bone defects, that are diagnostically distinguishable from the signs of infection-driven peri-implantitis.¹³ Finally, a systematic approach to management, integrating risk assessment, force-attenuating prosthetic design, and mandatory protective appliance therapy, is essential for improving the long-term prognosis in this high-risk population.¹³
6.2 The Imperative for a Proactive Stance
In clinical practice, academic uncertainty cannot be a justification for inaction. While researchers continue to elucidate the exact cellular mechanisms of bone response to overload, clinicians are faced with the practical reality of treating bruxing patients every day. The overwhelming weight of clinical correlation and the documented cascade of mechanical failures mandate a conservative and proactive approach. The guiding principle must be one of evidence-based precaution. Clinicians should assume that unmanaged bruxism will, over time, lead to complications. Therefore, the implementation of a comprehensive management strategy, as outlined in this report, should be considered the standard of care for these patients. It is noteworthy that while major professional bodies like the American Dental Association (ADA) and the European Association for Osseointegration (EAO) have provided consensus definitions for bruxism and general principles for implant care, specific, detailed clinical practice guidelines for managing bruxism in implant patients have yet to be established.⁴³ This places the responsibility squarely on the evidence-informed clinician to synthesize the available research and apply it judiciously to protect their patients' health and investment.
6.3 Future Directions: The Path to Clarity
The path toward resolving the remaining controversies and refining treatment protocols lies in future research. The single greatest need is for the development and widespread adoption of standardized, quantifiable, and repeatable methods for measuring occlusal forces in the clinical environment.²⁶ The current reliance on subjective proxies for overload, such as wear facets, is a major limitation in the research.³⁰ The integration of digital occlusal analysis tools that can provide objective data on force magnitude, timing, and location holds immense promise. Large-scale, long-term clinical trials utilizing these technologies could finally help establish definitive force thresholds for bone damage and component failure. This would allow the field to move from generalized, intuitive guidelines to truly customized, patient-specific risk assessment and prosthetic design, ultimately resolving the bruxism conundrum and ensuring the highest possible long-term success for all implant patients.
Works cited
Relation between bruxism and dental implants - SciELO, accessed July 1, 2025, https://www.scielo.br/j/rgo/a/QLwd879p4YJNdSDc4wTT5Dq/?format=pdf
Relation between bruxism and dental implants - SciELO, accessed July 1, 2025, https://www.scielo.br/j/rgo/a/QLwd879p4YJNdSDc4wTT5Dq/?lang=en
Failed Dental Implant – What Are My Options? - Chesterfield Dentistry, accessed July 1, 2025, https://www.chesterfielddentistry.com/post/failed-dental-implant-what-are-my-options
Implant for Posterior Molar with Parafunctional Habit; Cautious Approach, accessed July 1, 2025, https://pubs.sciepub.com/ijdsr/3/4/6/index.html
Intricate Assessment and Evaluation of Effect of Bruxism on Long-term Survival and Failure of Dental Implants, accessed July 1, 2025, https://www.thejcdp.com/doi/10.5005/jp-journals-10024-1910
Bruxism: Its multiple causes and its effects on Dental Implants: A Review, accessed July 1, 2025, https://www.craniofacialjournal.com/articles/johcs-aid1012.php
(PDF) Dental implants in tooth grinders - ResearchGate, accessed July 1, 2025, https://www.researchgate.net/publication/8643573_Dental_implants_in_tooth_grinders
Can Dental Implants Fail Due to Bruxism or Teeth Grinding?, accessed July 1, 2025, http://www.shoresmilesdentalny.com/can-dental-implants-fail-due-to-bruxism-or-teeth-grinding
Is Bruxism a Barrier to Getting Dental Implants? - St. Charles Family Dentistry, accessed July 1, 2025, https://www.stcharlesdentist.com/is-bruxism-a-barrier-to-getting-dental-implants/
Occlusion and Biomechanical Risk Factors in Implant-Supported Full-Arch Fixed Dental Prostheses—Narrative Review - PubMed Central, accessed July 1, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC11856061/
Occlusal overload with dental implants: a review - PMC - PubMed Central, accessed July 1, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC6646429/
Identifying occlusal overload and how to deal with it to avoid marginal bone loss around implants - ResearchGate, accessed July 1, 2025, https://www.researchgate.net/publication/230571486_Identifying_occlusal_overload_and_how_to_deal_with_it_to_avoid_marginal_bone_loss_around_implants
Bruxers to Bone Loss working.pdf
Does traumatic occlusal forces lead to peri-implant bone loss? A systematic review - SciELO, accessed July 1, 2025, https://www.scielo.br/j/bor/a/YgBH93p8tMQ74Z39CNZPzqg/
Bruxism and the Risk of Dental Implant Failure - International Journal of Prosthodontics and Restorative Dentistry, accessed July 1, 2025, https://www.ijoprd.com/doi/10.5005/jp-journals-10019-1368
Dental Implant Failure Risk in Patients with Bruxism—A Systematic Review and Meta-Analysis of the Literature - PubMed Central, accessed July 1, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC11763436/
Implant complications in bruxism patients - Journal of the Korean Association of Oral and Maxillofacial Surgeons, accessed July 1, 2025, https://www.jkaoms.org/journal/view.html?doi=10.5125/jkaoms.2021.47.2.149
International consensus on the assessment of bruxism: Report of a work in progress - PubMed, accessed July 1, 2025, https://pubmed.ncbi.nlm.nih.gov/29926505/
Bruxism: An umbrella review of systematic reviews - PubMed, accessed July 1, 2025, https://pubmed.ncbi.nlm.nih.gov/30993738/
Teeth Grinding: You Won't Believe How Harmful it Really Is | Health.mil, accessed July 1, 2025, https://health.mil/News/Articles/2022/02/28/Teeth-Grinding-You-Wont-Believe-How-Harmful-it-Really-Is
Teeth Grinding | MouthHealthy - Oral Health Information from the ADA, accessed July 1, 2025, https://www.mouthhealthy.org/all-topics-a-z/teeth-grinding
Does traumatic occlusal forces lead to peri-implant bone loss? A systematic review - SciELO, accessed July 1, 2025, https://www.scielo.br/j/bor/a/YgBH93p8tMQ74Z39CNZPzqg/?format=pdf&lang=en
Bruxism and dental implants: A systematic review and meta‐analysis - Dental24, accessed July 1, 2025, https://dental24.se/wp-content/uploads/2023/09/joforalrehabilitation-2023-hggmanhenrikson-2.pdf
(PDF) Prevalence and predictors of bruxism in two university clinic patient populations with dental implants: A cross-sectional analysis - ResearchGate, accessed July 1, 2025, https://www.researchgate.net/publication/360426837_Prevalence_and_predictors_of_bruxism_in_two_university_clinic_patient_populations_with_dental_implants_A_cross-sectional_analysis
Occlusal overload with dental implants: a review - ResearchGate, accessed July 1, 2025, https://www.researchgate.net/publication/334636948_Occlusal_overload_with_dental_implants_a_review
Peri-Implant Bone Loss and Overload: A Systematic Review Focusing on Occlusal Analysis through Digital and Analogic Methods - MDPI, accessed July 1, 2025, https://www.mdpi.com/2077-0383/11/16/4812
Occlusal overload and bone/implant loss | Request PDF - ResearchGate, accessed July 1, 2025, https://www.researchgate.net/publication/232715159_Occlusal_overload_and_boneimplant_loss
Occlusal overload and bone/implant loss, accessed July 1, 2025, https://acodent.academy/wp-content/uploads/2024/07/%D9%85%D9%82%D8%A7%D9%84%D9%87-23.pdf
Impact of excessive occlusal load on successfully-osseointegrated dental implants: A literature review - ResearchGate, accessed July 1, 2025, https://www.researchgate.net/publication/255689984_Impact_of_excessive_occlusal_load_on_successfully-osseointegrated_dental_implants_A_literature_review
Peri-Implant Bone Loss and Overload: A Systematic Review ..., accessed July 1, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC9409652/
Peri-Implant Bone Loss and Overload: A Systematic Review Focusing on Occlusal Analysis through Digital and Analogic Methods - PubMed, accessed July 1, 2025, https://pubmed.ncbi.nlm.nih.gov/36013048/
Is bruxism a risk factor for dental implants? A systematic review of the literature - PubMed, accessed July 1, 2025, https://pubmed.ncbi.nlm.nih.gov/23151302/
Dental Implant Failure Risk in Patients with Bruxism—A Systematic Review and Meta-Analysis of the Literature - MDPI, accessed July 1, 2025, https://www.mdpi.com/2304-6767/13/1/11
Does Bruxism Contribute to Dental Implant Failure? A Systematic Review and Meta-Analysis, accessed July 1, 2025, https://pubmed.ncbi.nlm.nih.gov/25726844/
Bruxism and dental implant failures: a multilevel mixed effects parametric survival analysis approach - PubMed, accessed July 1, 2025, https://pubmed.ncbi.nlm.nih.gov/27611304/
Risk of Dental Implant Failures May Be Higher in Bruxers Than Nonbruxers - PubMed, accessed July 1, 2025, https://pubmed.ncbi.nlm.nih.gov/38821662/
Long-term Retrospective Study based on Implant Success Rate in ..., accessed July 1, 2025, https://thejcdp.com/doi/JCDP/pdf/10.5005/jp-journals-10024-2217
Bruxism and dental implant failures: a multilevel mixed effects parametric survival analysis approach, accessed July 1, 2025, https://yehhsinchi.com/wp-content/uploads/2016/11/journal-of-oral-rehabilitation-2016-vol-43-p-813-823.pdf
Clinical Appearances of Dental Implant Overload and Precautions | Madridge Publishers, accessed July 1, 2025, https://madridge.org/journal-of-dentistry-and-oral-surgery/mjdl-1000117.php
Bruxism Management - StatPearls - NCBI Bookshelf, accessed July 1, 2025, https://www.ncbi.nlm.nih.gov/books/NBK482466/
Dental Implants and Bruxism: What You Need to Know, accessed July 1, 2025, https://newteethchicagodentalimplants.com/dental-implants-and-bruxism-what-you-need-to-know/
Interventions for replacing missing teeth: different times for loading dental implants, accessed July 1, 2025, https://www.cochrane.org/CD003878/ORAL_interventions-for-replacing-missing-teeth-different-times-for-loading-dental-implants
Clinical Practice Guidelines and Evidence - American Dental Association, accessed July 1, 2025, https://www.ada.org/resources/research/science/evidence-based-dental-research
Statement on Dental Implant Practices in the News, accessed July 1, 2025, https://www.ada.org/about/press-releases/statement-on-dental-implant-practices-in-the-news
European Association for Osseointegration, accessed July 1, 2025, https://eao.org/
EUROPEAN JOURNAL OF - Foundation for Oral Rehabilitation, accessed July 1, 2025, https://www.for.org/sites/default/files/2018-09/Consensus-on-the-avoidance-and-management-of-complications-of-implant-based-treatment-Foundation-for-Oral-Rehabilitation_rev.pdf